Eyewitness reports: Cholera on the march again
With oral cholera vaccine (OCV) in short supply, keeping the lid on cholera outbreaks is proving ever more difficult.
- 4 April 2024
- 6 min read
- by Ian Jones , Charlotte Mbuh

Cholera has long been a scourge of humankind. Since the early 1800s, seven pandemics have swept the globe, killing millions. The most recent pandemic, starting in 1961, is still ongoing, ebbing and flowing. Now, a combination of factors, including poverty and climate change, are driving a surge in outbreaks – affecting at least 29 countries, from Afghanistan to Zimbabwe.
Not only are there more outbreaks, they are also getting larger. The crisis shows little sign of abating: the number of cholera cases more than doubled between 2021 and 2022 to 473,000, and preliminary data suggests another large jump in cases in 2023, causing more than 5,500 deaths since the start of 2023.
Cholera is spread mainly through contaminated water, so improving sanitation and providing access to clean water is ultimately the best route to prevention. Over the short term, vaccination can provide a high degree of protection. Unfortunately, the recent surge in cases, coupled with limited global OCV manufacturing capacity, has meant that global demand for OCV vastly exceeds supply.
OCV was one of the topics covered at the eighth Teach to Reach: Connect event organised by the Geneva Learning Foundation (TGLF), the report from which has just been published. Teach to Reach events provide an opportunity for health workers from the Global South to share their experiences with their peers, enabling them to learn from each other.

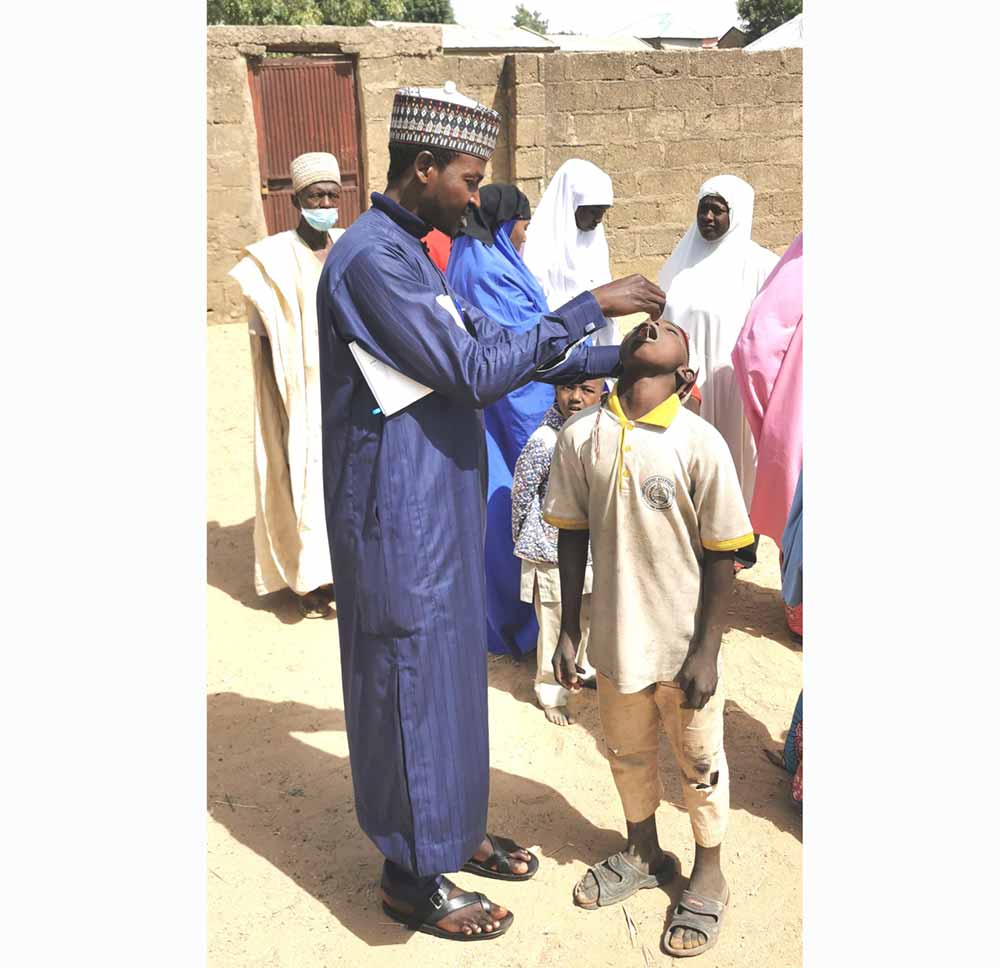
Credit: Aliyu Muhammad/Movement for Immunization Agenda 2030
Many respondents highlighted how global supply shortages had affected local OCV programmes. Some programmes have switched to use of single-dose OCV, rather than the usual two-dose schedule, as recommended by the International Coordinating Group (ICG), the global body that coordinates distribution of OCV. Single-dose OCV is sufficient to provide immediate protection, but this protection is not as long-lasting as after two doses. Respondents also noted that difficult decisions must be made about which groups should receive limited supplies of vaccine.
"The main targets for vaccination are populations at high risk of exposure to cholera, based on analysis of previous epidemics. If the number of vaccines available is limited, only particularly vulnerable sub-populations (preschool or school-age children, pregnant women, people infected with HIV and the elderly) can be selected because of a particularly high risk of infection and/or mortality."
– Martince Yuma Zahera, Community Health Worker, Facility-level, DRC
Contributors shared detailed strategies and plans for outbreak control. OCV delivery strategies include fixed teams, mobile teams and door-to-door approaches. Use of OCV is typically within integrated campaigns, which require coordination across different authorities and are dependent on good working partnerships and effective micro-planning. Campaigns are often associated with efforts to improve access to clean water or to provide methods of water purification.
"We moved door to door and also carried out advance fixed vaccination strategies and distribution of aqua tablets, and also disinfected wells and other risk areas."
– Dr Ndifontiayong Adamu Ndongho, Ministry of Health, District-level, Cameroon
Challenges included reaching displaced or mobile populations, who are typically at heightened risk of cholera, as well as practical issues such as the size of boxes used for transportation and distribution – a reminder of the practical daily challenges health workers face.
"The main challenge was how bulky it was; for those facilities with small fridges, the storage was a challenge."
– Mary Wanjiru Kamau, Nurse, Ministry of Health, District-level, Kenya
Have you read?
Although OCV is generally used in outbreak settings, contributors noted that there was still some resistance to its use in communities and concerns about its safety. With cholera outbreaks occurring during the COVID-19 pandemic, there were widespread concerns that OCV campaigns were a ploy to smuggle in COVID-19 vaccine.
"The cholera vaccine was rejected by many on the pretext that it was the same as the COVID-19 vaccine, but presented in a different form."
– Lamine Mahamat Seid, Community Health Worker, Ministry of Health, National-level, Chad
Respondents shared a variety of strategies they had used to build confidence and encourage uptake of OCV. Engaging with community leaders and other influential figures was seen as a key way to build community support.
We began by working with the local traditional guardians to demonstrate the benefits of the vaccine and the results it has produced in other places. We explained to them that, like all vaccines, OCV can have minor side-effects that disappear in less than 48 hours, but if there are any serious manifestations, our services will be able to deal with them in the nearest health facilities. By mutual agreement, we decided to start getting vaccinated ourselves, in front of the public, the local political and administrative authorities, and the family members of the vaccination teams. This aroused a desire to be vaccinated among our target populations and, in the end, our results were satisfactory because we had maintained constant communication using all the channels accessible to each community."
– Ouedraogo Lassane, Ministry of Health, National-level, Burkina Faso
As noted above, self-administration of OCV was also highlighted as one way to assure communities about the safety of the vaccine. Other strategies discussed included communicating the consequences of catching cholera and making use of trusted community health workers to engage with communities.
Credit: Muslim Muhammad Ladan Maru/Movement for Immunization Agenda 2030
"We had challenges with parents who refused to take the vaccines and in turn prevented their children from doing the same. We had to convince them of the importance of the vaccine by first making them perceive the severity of the outbreak, showing them case fatalities and pictures of persons suffering, and also using community health workers whom they trust to better school them on the importance of vaccination."
– Ilunga Kikunga Jean Paul, Ministry of Health, District-level, DRC
Engaging with communities was also seen to have other benefits, for example by providing an opportunity to stress the importance of good water, sanitation and hygiene (WASH) practices to prevent the transmission of disease. Activities discussed included innovative use of drama to engage audiences.
"Enablers included good social mobilisation, working with community leaders, good microplanning, political will from the local authority, supportive supervision, good data management plan, continuous daily coordination meeting and proper communication."
– Samuel Majang Mut, Ministry of Health, Region-level, South Sudan
With only one manufacturer currently producing OCV, shortages are likely to persist. In the medium term, efforts are being made to transfer technology to additional manufacturers, to increase the volume of vaccine being produced. And in the longer term, improved sanitation and access to clean water will be the most effective route to cholera control.
In the meantime, connecting health workers trying to deal with cholera outbreaks can be a valuable way to facilitate the sharing of experiences and practical advice, to help them make the best of a difficult situation.
Learn more:
- Download the Teach to Reach 8 report: Jones, I., Eller, K., Mbuh, C., Steed, I., & Sadki, R. (2024). Making connections at Teach to Reach 8 (IA2030 Listening and Learning Report 6) (1.0). Teach to Reach: Connect 8, Geneva, Switzerland. The Geneva Learning Foundation. https://doi.org/10.5281/zenodo.8398550
- View WHO cholera and acute watery diarrhoea dashboard.
- Learn more about the Movement for Immunization Agenda 2030 and Teach to Reach.
More from Ian Jones


![Bouaké, Cote d'Ivoire [Credit: TGLF]](/sites/default/files/vaccineswork/2024/Header/Bouake_panoramio_h1.jpg)
Recommended for you





