Q&A: Religious minorities and ‘faith’ in vaccines
Nurturing confidence in vaccination among minority populations like the Haredim, a Jewish religious group sometimes problematically referred to as “ultra-Orthodox,” has a lot to do with listening, says medical anthropologist Ben Kasstan.
- 27 January 2022
- 11 min read
- by Maya Prabhu
“From Jerusalem to New York to London,” wrote University of Bristol medical anthropologist Dr Ben Kasstan of the early months of the pandemic, “I noticed a common thread in new reports that homogenized the so-called ultra-Orthodox Jewish minority as noncompliant with – if not obstinate to – public health control measures.”
Haredim – which means “God-fearing” – are deliberately self-protective and cautious of forces they understand as undermining to that stance – especially influences perceived as ‘secular’. But when it comes to public health, and in particular vaccine decision-making, religiosity does not preclude “secular” concerns. Our conversation with Kasstan, edited for clarity and concision, follows below.
The language of “religious exemption” creates a kind of myth that it's religious beliefs that are the source and the root of opposition [to vaccination] in religious minorities. And I haven’t found that to be true.
VW: Let’s dive in. Why are we talking about vaccination among Haredi Jewish minorities? What brought you to this subject?
BK: There tends to be a pattern of suboptimal vaccination coverage among Haredi Jews in the US, Israel and the UK. The measles outbreaks of 2018 to 2019 were linked to Haredi Jewish neighbourhoods and quickly spread across local, regional, national and international boundaries. The US and Israel ended up having the biggest measles outbreaks in a quarter century. So, actually, we’re not talking about a kind of “minority health” issue. Understanding these patterns and events have really got broader implications
I’m an anthropologist, which means I conduct long-term research with populations to produce theoretical questions, but also to think about practical implications, and in this case, around vaccinations. Coming from a Jewish background, I was always really intrigued that there was a part of the population called Haredim who were framed as “hard to reach” by public health services in various countries, often because of suboptimal vaccination coverage. So I was really curious to understand what that means – “hard to reach” – and the kind of values-based judgements around that term, and terms like “compliance”, you know, as in “non-compliant community”.
What I found [during my PhD research] is that rather than being “hard to reach,” we’re talking about health care, and health care is one of the few remaining places where this minority and the state actually interact and negotiate each other’s positions. So “hard to reach” didn’t really seem to reflect what was going on.
© The Queen’s Nursing Institute
VW: You quickly dismiss is the idea that there exists, for this group, a general theological position against vaccination, the sort of thing one imagines as furnishing a “religious exemption”. You speak to plenty of Haredim who are eager to vaccinate their children. Can you tell us a bit more about the distortive assumptions that orbit this idea of “religious exemption”?
BK: So the language of “religious exemptions” is really something specific to the US, in their kind of vaccination policies and, you know, the kind of sacred place of religious freedoms in the US – or their interpretations of religious freedoms. But that discourse gets exported more broadly and in quite problematic ways.
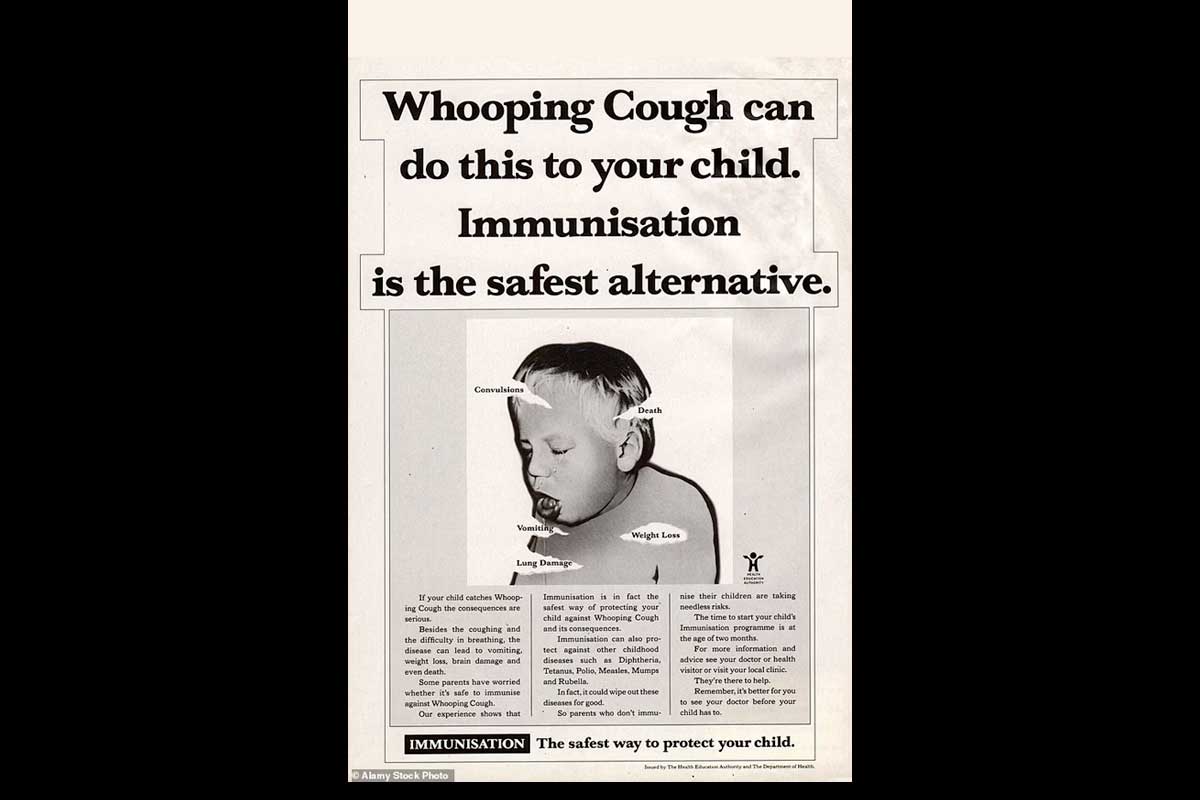
Having had these conversations around childhood vaccinations with Haredi Jewish parents, you see that actually, their concerns and their decisions are very much in line with the broader population’s. Is this the safest way to protect my child? Is this the right time? You know – our children’s bodies are specific, and their immune systems are specific to them, not generalisable like a vaccination programme suggests.
This language of “religious exemption” creates a kind of myth that its religious beliefs that are the source and the root of opposition [to vaccination] in religious minorities. And I haven’t found that to be true.
Have you read?
VW: You find that religious authorities don’t even necessarily have a dominant influence on parents’ decision-making about vaccination.
BK: I think that’s [an assumption] we see in lots of vaccination programme guidance, especially so in the global south – again, it almost essentialises the problem [of non-vaccination] as a religious belief issue, when the concerns are much broader, and the sources of consultation and information are different. Parents [in the Haredi population] rarely want to consult religious authorities on vaccination. Religious authority is one of the range of issues that needs to be considered, and it probably doesn’t do any harm to include religious figures in vaccination programmes. But focusing only on religious authorities probably does do some harm because it forecloses other ways of making decisions, and other sources of authority such as, for example, doulas or professionals working directly with women, as mothers are the primary decision-makers..
What we’re talking about are [parental] concerns around vaccine safety. And those concerns become consolidated in a kind of grammar of religious law – and that’s directly related to this legitimacy of “religious exemptions” because that’s what the law offers. But actually the root of that is not really about religion, it’s just consolidated in a way that makes that opposition legitimate. But first and foremost are questions around vaccine safety – and, kind of, the infiltration of non-vaccination advocacy, which as you know, is not always evidence-based and can be quite fear-mongering.
VW: Yeah, I was a little surprised, reading your work, that Andrew Wakefield’s long-debunked claims about the MMR vaccine show up in conversations with members of this quite insulated religious minority.
BK: There’s the legacy of Wakefield which I think accounts for “vaccine hesitancy” in lots of different populations, so there’s that – but we’re also talking about the circulation of non-vaccination messaging, between the US, Israel and the UK, with groups who are not Haredi, almost targeting these minority populations, with broader kind of religious claims – like vaccines like rubella being cultured on human cell lines. That’s exported from a Catholic set of concerns. These kinds of activists try to infiltrate these messages and these concerns into another context and try to convert, you know, those grammars to make them relevant to other populations.
Having done ethnographic field work since 2013, one of the really most concerning experiences of my life was going into a hotel in Jerusalem one night in November 2019, and going to an event that was held “in support of the vaccine injured community”, bringing activists from the US such as Del Bigtree, who had become a source of kind of authoritative knowledge among this group of vaccine-opposed religiously orthodox parents. .

Photo by Ami Dabush
VW: You’re not keen on the phrase “vaccine hesitancy”. Can you tell me why?
BK: More than anything, it tends to position people as problems – to put the emphasis on people rather than broader questions around structures and services, commissioning, programming. My feeling is that vaccine hesitancy is part of the story, but it’s not the definitive part of the story. And ultimately, vaccination services are there to serve – and that’s going to take different shapes and forms in different places.
There’s another question that often gets obscured in these conversations of “hesitancy” – and that’s convenience and access. Haredi families have got many children – I’ve met families of up to about 16 children – with women that are consistently pregnant until menopause. That’s going to affect, you know, your engagement with services, taking children to routine appointments. And again, something I’ve consistently encountered is that local providers are aware of this issue, but they are not always given the flexibility and support in terms of commissioning and programming to address these known concerns.
VW: Let’s talk about immunity. You write about the pursuit of multiple kinds of immunity – including political immunity and biological immunity – and how these immunity projects sometimes intersect to the detriment of human health.
BK: This is a population that tries to be immune from the outside world and outside influences. That means it’s going to have different ways of negotiating, for example, what is presented to them as the right, responsible thing to do. For example, the desire to be self-protective or to be “immune” from outside influences might affect your engagement with health information and what sources of information you view as authoritative. And there’s another question – in a context where the school curricula are limited, especially in terms of science, the kind of formative encounters around biology and immunology are not the same as in non-Haredi schools.
Ideas of what’s appropriate or authoritative are going to play out in different ways for different vaccination programmes. Religious populations were not accepting the HPV vaccine, for example, because it was a risk that was seen to face the broader population who were maybe having sexual relationships earlier, before marriage, multiple sexual partners, whatever. But in a population with its own kind of moral regulations around sexuality and relationships, this wasn’t seen as relevant.
COVID-19 was the largest vaccination programme, I think, in human history, developed and implemented at a record pace. That influenced the way it was implemented – and the kind of responses that were generated. So, in Israel, the COVID-19 vaccine programme was implemented, like in any other place, very quickly, and there were all these kinds of metaphors around protecting the “Jewish state” — and definitions of that can be excluding of Haredi populations and they may even exclude themselves. Even before the vaccination programme was implemented, you had the IDF [Israel Defence Force] involved in imposing public health control measures, including in Haredi cities, despite these long running tensions between that population and the state over the issue of military drafts* [*Haredi Jews hold a range of positions on Zionism and some may oppose or not explicitly endorse it. Haredi Jews are exempted, currently, from the otherwise almost universal draft into the army – a recurrent question of national political controversy.]
VW: You write about “autoimmunity” as a mechanism that might underpin some instances of resistance to COVID-19 vaccination programmes. Can you explain?
BK: This is building on debates in political philosophy, where protective defences are built beyond the anticipated risk, which creates an “autoimmune response” that, in effect raises more of a problem than the original threat. It’s where these protective mechanisms against the outside world had been built so high that it has almost kind of enabled the threat from within, in terms of enabling the virus to have such an impact.
To a certain extent, we see that happening in self-protective Haredi populations that were so disproportionately impacted by the pandemic, in terms of morbidity. I was part of a study at the London School of Hygiene and Tropical Medicine, led by Dr Michael Marks, where a Haredi community in London was found to have extremely high seroprevalence rates of COVID.

Photo by Ami Dabush
VW: So for public health systems, there’s a need to not, kind of, blunder into triggering that self-protective spike which might, for instance, cause people to resist vaccination because it’s actually associated with incursions by the state?
BK: There’s an issue here with not listening to each other. Again, when we use that term “hard to reach” it kind of positions the minority as recalcitrant, obstructive. I think we sometimes forget how cultural public health is – how it happens in Israel is wildly different to how it’s going to happen in the UK.
But public health relations are formed and shaped and reshaped amidst these long-running alignments between minorities and states. At the root of misunderstandings between services and minorities, is this not-listening, when it comes to ideas of protection. In a situation like an emergency that leads to the frictions that we’ve been seeing.
VW: In the COVID-19 crisis, the vaccines are the best tool we have for protecting human health. If there’s a messaging problem that’s preventing people from accessing them, from reaching out for those vaccines, then how do we best adjust?
BK: So I think it’s really about looking across the board at the project of health protection, and envisioning something that doesn’t raise the concerns that people raise about services. The political economy of healthcare and vaccination is an important consideration in promoting confidence. One Haredi mother in the UK explained that her confidence in the vaccination project was shaken by concerns about GPs’ incentives – she understood physicians to be financially rewarded for immunising more people. That’s part of the conversation as much as information campaigns.
It’s looking at the issues in particular contexts and understanding the opportunities and understanding how public health services themselves need to be supported with investment from central governments to provide them with the flexibility they need. And I think it’s embedding listening in a model of public health relations with minority populations, to understand how to work with each other.
VW: I’m curious whether you’ve come across examples of public health engagement that you found impressive in this way?
BK: There are different examples that maybe don’t tick all the boxes, but show the potential. In New York, following the measles outbreaks, there was a coalition of Orthodox Jewish nurses who tried to combat some of the myths that were being circulated, trying to promote confidence in childhood vaccination. I and Dr Tracey Chantler at the London School of Hygiene and Tropical Medicine were examining how public health services in London collaborated with Hatzola, which is a kind of Haredi Jewish ambulance service, to co-deliver the COVID-19 vaccine programme. By virtue of acting on convenience, [they were] promoting confidence. It was almost like a partnership in the project of health protection. It’s understanding how ideas like this can be broadened and given a ‘shot.’
 | Read more from Ben Kasstan:
|