Mauritania: how “desert vaccinators” track outbreaks among the dunes
In Mauritania’s Adrar region, vaccination teams travel hundreds of kilometres across dunes and rocky plains to reach nomadic families constantly on the move.
- 23 February 2026
- 6 min read
- by Yamina Bendaïda
At a glance
- From meningitis to measles, infectious disease epidemics have historically hit Mauritanian nomads disproportionately.
- A new vaccination initiative is seeking to change that, bringing vaccines straight to transient herder families. Even locating them can be a challenge. “To vaccinate a single child, costs can be very high,” says Mohamed Vall Abdellahi, Head of the National Health Information and Epidemiological Surveillance Service. “The logistics are enormous.”
- There are encouraging signs of progress. One nomad mother, Lalla, explained, “The children are vaccinated here, at home,” referencing her tent.
Thirty kilometres south of the historic town of Ouadane, the landscape stretches like an ocean of sand and stone. This is where Aamar and his family live. They have been nomads for generations. “We are from around Ouadane,” says the 55-year-old herder. “Sometimes we are close, sometimes we move farther away. Right now, we are 40 km from the town.”
For families like his, whose lives are shaped by the search for pasture and water, access to healthcare remains a persistent challenge. Health facilities are distant, travel is difficult and movements depend entirely on rainfall.

Credit: Yamina Bendaïda
Mauritania lies within the African “meningitis belt”, a band of 26 countries stretching from Senegal to Ethiopia where more than 470 million people live under the threat of recurrent epidemics. Historically, meningitis outbreaks – particularly those caused by meningococcus A – swept through the region every five to twelve years, with devastating consequences in areas with limited access to treatment.
In 2014, a nationwide vaccination campaign using MenAfriVac marked a turning point.
“We conducted a large campaign targeting people aged 1 to 29,” recalls Mohamed Vall Abdellahi, Head of the National Health Information and Epidemiological Surveillance Service. “Since 2014, we have not had a problem with meningococcus A. The campaign was costly, but extremely effective.”
Across the continent, MenAfriVac has been credited with preventing nearly one million cases of meningitis A. The success demonstrated that even in challenging environments, large-scale prevention was achievable.
2018: measles exposes a gap
Four years later, however, another outbreak revealed the limits of existing strategies. In 2018, Mauritania experienced a wave of measles.
“Nomadic populations were the most affected,” Abdellahi explains. “Vaccination was complicated for them. There was simply no accessibility.”
In vast pastoral zones between the Trarza and Brakna regions, there are no permanent villages and no fixed health structures. For mobile populations, distance translates directly into vulnerability. The outbreak acted as a wake-up call for health authorities.
“The health services came and decided to strengthen vaccination for nomads,” he says. “The objective was clear: if nomads cannot come to vaccines, vaccines must go to nomads.”
Designing a strategy for the desert
Reaching families who move with seasons and rainfall presents formidable logistical challenges.
“To vaccinate a single child, costs can be very high,” Abdellahi admits. “The logistics are enormous.”
Health authorities therefore developed a tailored approach combining field intelligence, adapted cold chain solutions and strong community engagement.

Credit: Yamina Bendaïda
The first challenge is locating the camps.
“We don’t leave until we have precise information,” says one vaccinator. Teams gather intelligence in nearby settlements, sometimes travelling up to 200 kilometres to collect details about nomadic movements. Another opportunity arises when herders visit supply points.
“We meet them when they come to buy sugar, tea or other essentials. That’s when we identify where they are staying.”
Maintaining vaccine potency under Saharan heat is the next hurdle. “Heat is the vaccine’s number one enemy,” the vaccinator explains.
Have you read?
To overcome this, teams rely on high-performance insulated thermoses capable of preserving vaccines for up to seven days. These containers remain inside air-conditioned vehicles. Health workers carry only a small vaccine carrier during each visit. “I know exactly where the vial is. I minimise how long the thermos stays open.”
Equally crucial is the human dimension. “We never go alone,” the vaccinator says. “We always travel with someone who knows the tribe.”
Local guides act as cultural intermediaries, helping establish trust. Their presence often determines whether a visit succeeds. The arrival of the team is usually welcomed,” he adds. “It’s not only vaccination. We can also provide consultations and basic medicines.”
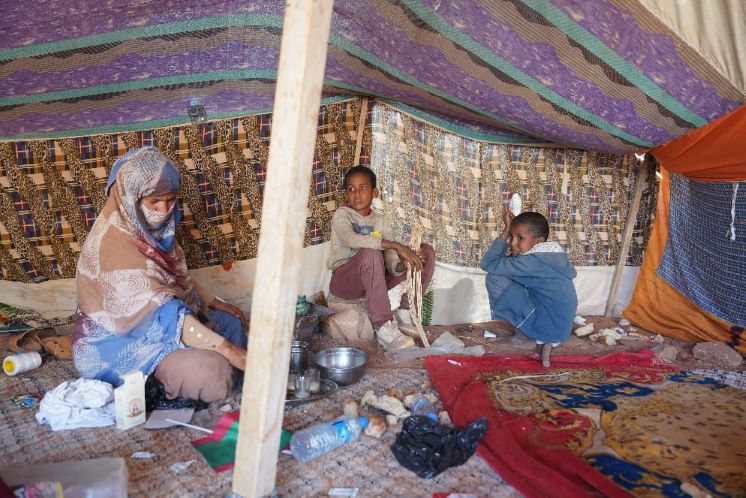
Vaccination under the tent
For Lalla, a 47-year-old mother of three, the mobile strategy has transformed access to care. “We live far from town,” she says. “When it’s time for vaccines, the teams come to us.”
The consultation and vaccination take place directly inside the family tent. “The children are vaccinated here, at home,” Lalla explains. “The team travels with all their equipment.”
Her children receive protection against tuberculosis (BCG), polio, tetanus and measles. Minor side effects are familiar. “The little ones sometimes develop a fever, but it’s not serious.”

Credit: Yamina Bendaïda
Challenges remain
Despite clear progress, significant obstacles persist. The primary difficulty remains the unpredictability of nomadic movements.
“We tried to establish migration calendars,” Abdellahi says. “But it was impossible. Everything depends on rainfall, which is highly irregular.”
Coverage gaps remain another concern. Some groups are still missed. “The teams only brought vaccines for children,” Aamar notes. He also raises a separate issue: livestock diseases, which can devastate livelihoods.
One kilometre at a time
Mauritania’s approach to vaccinating nomadic populations illustrates the degree of adaptation required to deliver immunisation in highly mobile, geographically dispersed settings. Through logistical innovation, flexible deployment and sustained community engagement, vaccination teams are extending protection into some of the country’s most isolated regions.
The path to universal coverage remains long. But each child vaccinated under a tent in the Sahara represents a small yet tangible step toward that goal.






