Meet the Abuja farmer who became a health worker to save his village
In a neglected primary health centre within Nigeria’s administrative capital, a farmer-turned-health worker volunteers to provide healthcare for the people.
- 9 April 2026
- 7 min read
- by Afeez Bolaji

At a glance
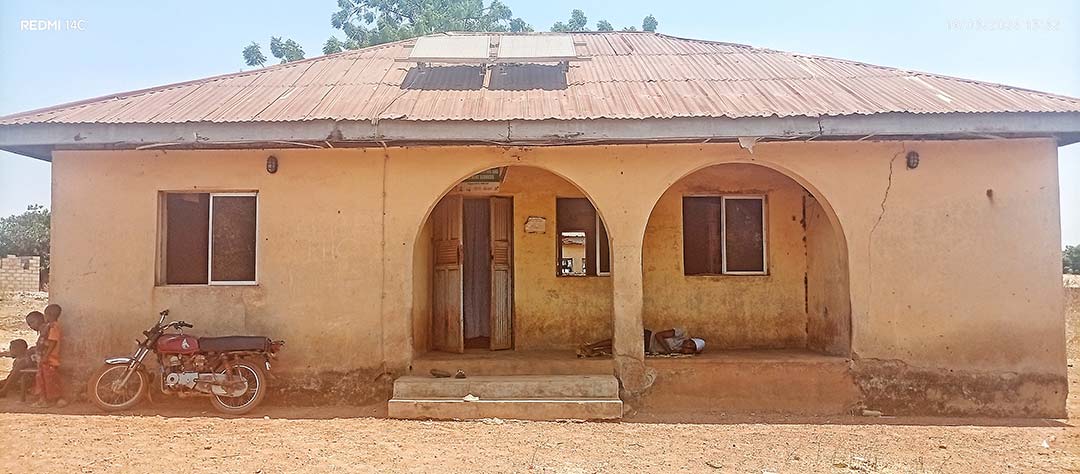
- Kigbe Primary Health Centre on the rural outskirts of Abuja is little more than a skeleton: dilapidated, under-equipped and perennially under-staffed. It’s also responsible for the care of about 2,000 people.
- A few years ago, one local farmer decided to fill the healthcare gap, and went off to study community health. Now he volunteers, day in, day out. “I act as the midwife, immunisation officer, community health extension worker and more. I usually go to the farm in the evening if there is not much work to do at the clinic,” says Usman Sirajo.
- Sirajo’s efforts mean that about 20 children who might otherwise go unprotected are immunised each week with the free vaccines that are sent regularly by local health authorities.
The odds are seemingly stacked against any health worker posted to Kigbe Primary Health Centre. The facility, which sits somewhat eerily on the outskirts of the Federal Capital Territory (FCT), Abuja, is dilapidated, under-equipped and perennially short-staffed.
But Usman Sirajo, a farmer turned community health volunteer, is defying all odds to make sure Kigbe, a village of about 2,000 people, does not go without essential health services. For routine maternal and child care, uncomplicated births, simple medical testing and minor treatments, 32-year-old Sirajo is on hand to lend a hand.
Credit: Afeez Bolaji
At 08:00 on a Thursday in late March, Sirajo was already at work setting up for the weekly routine immunisation session when nursing mothers began to trickle in with their babies.
Before long, James Tanko, the only paid health worker at the PHC, joined him to give a brief health talk to the mothers before vaccination commenced. Tanko lives in another community, and makes it to the clinic about three times a week.
“I live far from the hospital. My pay is small and I can’t afford to go to work every day,” Tanko explained. “Even if I decide to pass the night at the hospital, there’s no mattress for me to sleep. It is also dangerous to sleep there because reptiles can crawl in from the open ceilings,” he explained.
So, more often than not, the community depends solely on Sirajo. “I‘m a farmer, but I spend most of my time attending to patients,“ he told VaccinesWork as he prepared for vaccination. “I act as the midwife, immunisation officer, community health extension worker and more. I usually go to the farm in the evening if there is not much work to do at the clinic.”
Two hours into the exercise, no fewer than 16 children had received immunisations, ranging from BCG, OPV and Penta to yellow fever and measles vaccines.
“We immunise at least 20 children every Thursday. I always visit mothers whose children are due for immunisation to remind them of their next appointment date,” Sirajo explained during a short break, as he waited for more mothers to bring their children. “We also carry out immunisation outreach every two months. We inform pastors and imams ahead to announce the date to their congregation and we usually have a good turnout,” he added.
Sirajo’s efforts to repair compromised access to vaccination in this remote corner of Nigeria’s federal capital territory (FCT) is part of a bigger regional narrative.
World Health Organization and UNICEF estimates pegged coverage with even the first dose of the basic diphtheria, pertussis and tetanus-containing vaccine at just 71% nationwide in 2024, meaning that almost 30% of children in Nigeria remained unprotected from vaccine-preventable disease.
Government statistics suggest that Abuja and its environs lag behind the national average on immunisation. Records from the National Health Management Information System (NHIMS) put the percentage of children in the FCT who were fully immunised by age one at 76.5% in February 2026, compared to the national rate of 78.8% during the same period.
Propelled by cholera outbreak
Sirajo grew up here, in the capital’s agrarian hinterland. He took to farming at a young age, like many in Kigbe, helping his parents on their farm on weekends and during school holidays. That path seemed all but settled.
But he also recalls dreaming of becoming a doctor, an aspiration that grew stronger after a cholera outbreak swept through the community in 2014.
“We lost some people that year to the outbreak,” Sirajo remembers. But studying for a full medical degree was expensive, and his family couldn’t afford it.
Still, he says, “I was eager to fill the gap in the healthcare of our community. I decided to study community health at a college of health, and graduated.”
Have you read?
Sirajo says he has been volunteering at the local PHC since 2020 due to the shortage of staff, which has been a persistent challenge ever since the hospital was built over 20 years ago.
“Most health workers posted here left within a short period because it is a remote area without electricity and other basic infrastructure,” he says.
“For now, there is only one permanent health worker employed by the local government council and he lives in the neighbouring community. I handle emergencies alone, especially at night, but if the case is complex, I refer immediately to a higher hospital. I need more training, particularly in paediatrics, to better serve the community,“ he stated.
Inside the ageing PHC
Kigbe PHC lacks the basic needs of a functional primary health centre. Cracked walls, tattered ceilings, poor beds, a non-functional toilet, zero running water system, a chronic staff shortage, lack of essential drugs and a dearth of medical equipment mar the facility. A low-capacity solar system generates the only electricity that runs to the building, and it only suffices to powers a few ceiling lights.
“We need minor surgical tools, a nebuliser, an oxygen cylinder and regulator, an ECG machine, delivery kits and so on. The hospital also needs to be renovated and well-staffed. In the third trimester, we write all the necessary items to be used during delivery and ask the expectant mothers to get them ready because they are not available in the hospital.
“For families who can’t afford to get those items, some community members contribute to buy them. An organisation installed the solar power, but it could only light up the bulbs in the hospital,” Sirajo explains.
It is, however, not all doom and gloom, he says. “We get vaccines from local health authorities. They also gave us a solarised fridge that helps to store vaccines at the appropriate temperature.”
“Some officials visited early this year to assess the state of the hospital and promised to take action,” he added.
Locals relive encounters with Sirajo
Several residents interviewed by VaccinesWork commended Sirajo for what they described as a selfless public service.
Aisha Stephanus, who brought her six-month child for immunisation in March, spoke glowingly of how the volunteer went the extra mile to provide her antenatal care right from the first trimester until she gave birth.

Credit: Afeez Bolaji
“He was monitoring my progress and ensured that I came for antenatal care regularly,” she said. “He tries all his best to take care of the people in this community despite his limited resources and the poor state of the hospital. I went into labour at night and was rushed to the hospital.
“My husband put a call to Sirajo and he arrived within five minutes. He took the delivery safely and ensured that I bring my baby for immunisation afterwards. I imagine what would have happened in some cases if he was not available because his colleague lives in another community and is only available during the day,” she said, adding that she thinks he would be better able to look after the community if the hospital was upgraded.
Titus Luka, a community youth leader, recalled how Sirajo saved a woman who was suffering a miscarriage.
“She was rushed to the hospital at dead of night and had lost much blood. Sirajo showed up quickly and attended to her. He called his colleague, but his mobile phone was switched off. Thankfully, he was able to manage the case alone successfully,” Luka recalled.
People like Sirajo are critical to FCT health authorities’ efforts to reduce the maternal mortality rate, which dropped to 315.3 per 100,000 in February 2026 from 443.4 per 100,000 in 2024. The percentage of pregnant women who visited health centres for antenatal care (ANC) at least once rose to 47.8% during the period from 24.7% in 2024, while ANC coverage of four visits went up to 24.6% from 14.8% in 2024.
More from Afeez Bolaji



Recommended for you





