
yearsGavi@20
The story of an Alliance that today
protects half the world’s children
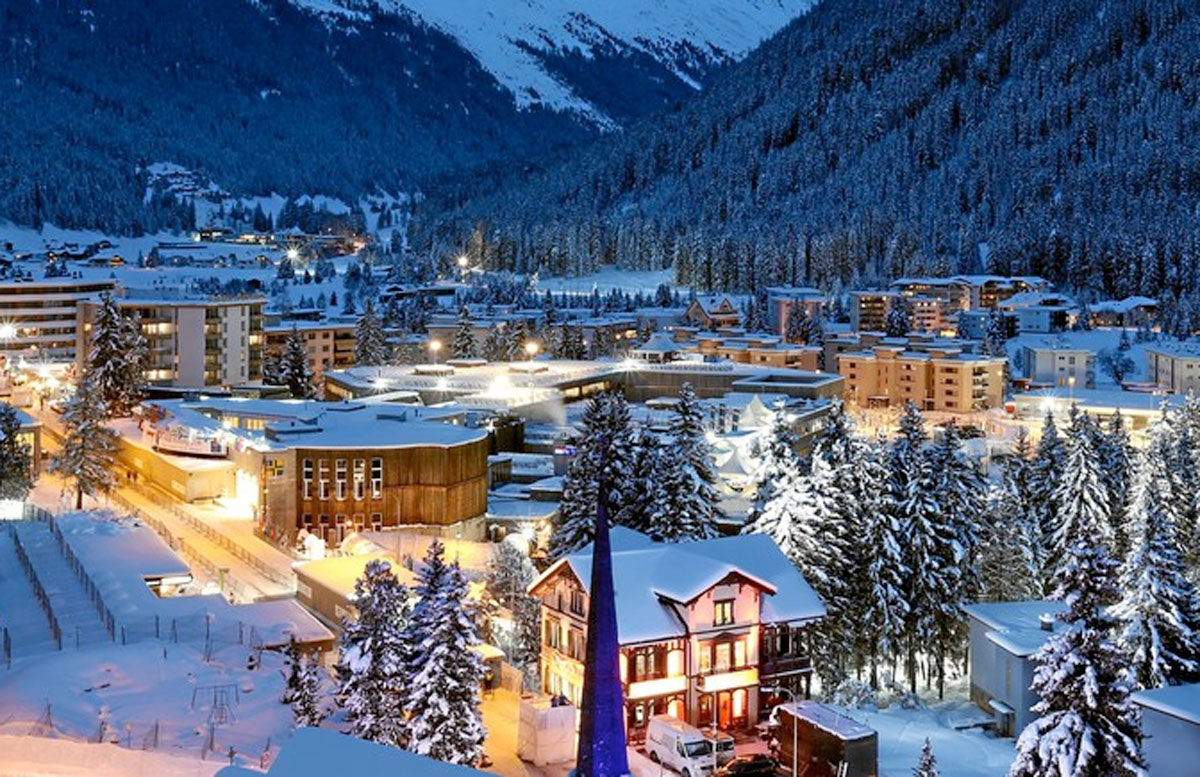
In 2000, a new kind of global health organisation was born. Launched at the World Economic Forum Annual Meeting in Davos, this new alliance sought to protect the most vulnerable children in the world from preventable infectious disease.
In two decades, its mission to save lives, reduce poverty and protect the world against the threat of epidemics has led it to help vaccinate more than 760 million children in the world’s poorest countries and prevent more than 13 million deaths. This is the story of how that organisation, Gavi, the Vaccine Alliance, came to be.
HOW AN AUDACIOUS IDEA LED TO A HEALTHIER GENERATION

1. The Origins of Gavi
This is the story of an audacious idea to solve an intractable problem. An idea that today helps protect almost half the world’s children against deadly and debilitating disease through vaccination. An idea which is now helping to save and transform the lives of millions of the most vulnerable individuals, to reduce poverty and boost the economies of the world’s poorest countries, and to make the world safer for everyone by reducing the threat of epidemics. This is the story of how that idea emerged, how it grew and how it succeeded.
Twenty years ago, a handful of committed people from very different backgrounds came together and discovered that they shared an ambitious vision: to deliver new and powerful vaccines, and provide children everywhere with protection from infectious diseases. The result of their hard work to overcome these challenges is Gavi, the Vaccine Alliance. More importantly, the result is a generation of children who are much more likely to survive and thrive into adulthood than any generation that has come before. Since 1990, the number of children under five who die each year, and the mortality rate for children in this age group, have both fallen by more than half – at least in part thanks to the spread of immunisation in low-income countries.
The birth of this remarkable Alliance was announced in the Swiss mountain resort of Davos in January 2000. But the story begins long before that, when a group of health scientists, politicians, philanthropists and industrialists began working on a shared set of challenges. As they confronted seemingly insurmountable obstacles, they identified a common goal: they wanted children across the world to gain equally from the immense benefits of immunisation, with life-saving vaccines reaching more people, in more countries, more quickly than ever before.

2. The vision takes shape
2. The vision takes shape
How a small group of people sought to find a solution to an urgent global health challenge that was preventing millions of children in poor countries from getting the protection they needed.
Read chapter 2
The story begins with an urgent global health challenge: children in poor countries were not receiving the vaccinations they needed, partly because of the way markets for pharmaceutical products were structured. The public health community was pushing for new vaccines to protect children in low-income countries against pneumonia and diarrhoea. Pharmaceutical companies had a clear response: you are not using the vaccines we already have, so why should we expend additional resources and effort to make new ones?
This highlighted a fundamental problem with global access to vaccines. Vaccines to protect children against deadly and debilitating childhood infections like Haemophilus influenzae type b (Hib)Haemophilus influenzae
Hib is a deadly bacterium which can cause meningitis, pneumonia and septicaemia. It’s the third-leading vaccine-preventable cause of death in under-fives, and it leaves up to 35% of survivors with disabilities. Although Hib vaccine had been available to wealthy countries since the 1980s, high costs meant low-income countries could not afford it (and only one had introduced Hib vaccine into its routine immunisation programme). So when Gavi was created in 2000, improving access to Hib vaccines in lower-income countries was an early priority, and so support for its introduction into routine immunisation programmes was immediately made available through Gavi. Today, all the world’s poorest countries protect against Hib through the Gavi-funded five-in-one pentavalent vaccine (see “Pentavalent”). and hepatitis BHepatitis B
Hepatitis B is a highly infectious virus – 50 times more infectious than HIV – that can cause liver cancer and cirrhosis. In 2000, fewer than 10% of low-income countries were using the vaccine that is 98% effective at protecting people against the virus. As a result, the infection was claiming an estimated 900,000 lives each year – most of them in low-income countries. At the time, only 22 low-income countries had access to a vaccine that protected against hepatitis B. Gavi supported introductions of the vaccine both separately and as part of the five-in-one pentavalent vaccine. Today, all Gavi-supported countries have introduced pentavalent vaccine, which includes hepatitis B. China was one of the first countries where the hepatitis B vaccine was supported by Gavi. By 2005, the government decided to include the vaccine in its routine immunisation programme. Hepatitis B introduction was an early test of the Gavi model and helped demonstrate that the Vaccine Alliance’s approach could rapidly accelerate the introduction of a new vaccine in low-income countries. were not reaching the children in low-income countries who needed them, while other critical vaccines were not even available in these countries. This failure of markets to deliver vaccines where they were most needed – or to develop equally vital new products – was the driving force that led, two years later, to the creation of what is now Gavi, the Vaccine Alliance.
The spirit of Gavi is partnership. We do things together. We bring giants in their own capacity from the multilateral, national, industry, civil society together, and instead of dominating, we are collaborating, and we create this higher unity that we couldn't have done apart.
Dagfinn Høybråten, former Chair, Gavi Board

For the small group of people working to put together the new alliance, the solution was to work with manufacturers to help them better understand the scope of vaccine markets in developing countries. Rather than focus on selling a few high-priced products to lower-income countries, the alliance aimed to demonstrate to industry the huge market potential for lower-priced products.
The founders of Gavi knew they needed a new approach: a broad new alliance, bringing together the interests and expertise of the World Health Organization (WHO), UNICEF, the World Bank and the private sector, to fix this market failure and deliver the benefits of vaccination to all children. It wasn’t the first time a public-private partnership had been attempted, but the level of commitment and support was unprecedented. Previous efforts to bring together different partners and address the challenges of universal immunisation had not achieved their goals. This time had to be different: a new approach, ambitious goals, and the game-changing funding to support them.

Twenty years ago, the children of the world weren't getting the vaccines they needed. The children at most risk in poor countries were the ones who were getting the least vaccines. And so we needed to find the resources to get countries to adopt the vaccines so that every child would be protected against diarrhoea, pneumonia and other killing diseases.
Bill Gates, Co-Chair, Bill & Melinda Gates Foundation
One of the first questions was where to find a new source of funding to support the scale of impact that was needed. In Seattle, Bill and Melinda Gates were thinking about where to concentrate their philanthropy and were increasingly focussing on the power and potential of vaccines. They had been reading about how the biggest killers of children in low-income countries, pneumonia and diarrhoea, were often caused by highly preventable infections, like pneumococcal disease and rotavirus, and they were keen to help find a solution.
Bill and Melinda Gates wanted to do something big, and the new vaccine alliance had the potential to achieve their goals. Their extraordinary donation provided the foundation on which to put these ambitious plans into practice.
The Gates Foundation announced a gift of 750 million dollars to support a new immunisation initiative. One of the UNICEF board members thought the translator made a mistake – it couldn’t be as much as 750 million. But it was, and it was amazing.
Carol Bellamy, Former Executive Director, UNICEF; Former Chair, GAVI Board

3. Going public
3. Going public
With the idea of how to solve this problem hatched, it was now time to go public, and to bring together the partners to form a new kind of alliance – the kind that was needed to turn the vision into a reality.
Read chapter 3
Even with the promise of high-level support and unprecedented funding, many challenges remained: how to align financing with operations; how best to engage with countries; how to ensure the equal participation of industry, governments and policy-makers. Other partnerships, alliances and organisations had failed because they did not take into account mutual suspicions and misunderstandings, even among groups ostensibly working for the same outcomes. There was also a reluctance among some about the new approach.

There was always this suspicion about the role of the private sector. I had to spend a lot of time convincing public servants in UNICEF and WHO that we needed to make drastic, innovative steps to make a real difference.
Gro Harlem Brundtland, former Director-General, WHO; founding Chair, GAVI Board
After many months of hard work and lengthy negotiations, the new alliance was ready for its public launch, and where better than the World Economic Forum Annual Meeting in Davos? The Forum had been created to bring together leaders from the public and private sectors to tackle some of the world’s greatest challenges. Increasingly, it was turning its attention to practical ways to solve global health problems.
The launch event brought together leaders from the United Nations, including Carol Bellamy of UNICEF, Gro Harlem Brundtland of WHO and James Wolfensohn of the World Bank; with those representing countries, like President Joaquim Chissano of Mozambique; the pharmaceutical industry, like Raymond Gilmartin of Merck; and philanthropists, like Bill Gates.
Gavi was one of the first major platform initiatives of the World Economic Forum. In many ways, it is a role model for how the public and private sector should cooperate to work in a much more efficient way, compared with the effect of governments alone or business alone or civil society alone.
Klaus Schwab, Founder and Executive Chairman, World Economic Forum

With the public launch done and ambitious commitments announced, it was time to turn the vision into reality. Early on, it was decided to separate the fundraising and policy parts of the alliance into two distinct organisations. The Global Alliance for Vaccines & Immunization (GAVI) took on the operational and policy work. Fundraising was in the hands of The Vaccine Fund; its first Chair was President Nelson Mandela, as his widow and the second Chair recalls.

Madiba has always been very passionate about children. … He always wanted children to have the best society could give. So, when he was approached to chair The Vaccine Fund, it was naturally something which gave him a platform to serve children globally.
Graça Machel, former Chair, The Vaccine Fund
President Mandela’s first task was to bring together other leaders to serve on the Board
President Mandela’s first task was to bring together other leaders to serve on the Board

I was serving as UN High Commissioner for Human Rights in the year 2000. I got a phone call from Nelson Mandela, and he asked me to serve on the GAVI Fund board, which had just been established, and he was Chair. And of course, when Mandela asks, you feel very honoured. So, I said yes, but I also was aware that we hadn't been successful in reaching children for vaccination. We needed to very much up that game.
Mary Robinson, former Chair, GAVI Alliance Board
It was undoubtedly challenging to bring together partners from public and private sectors, and from different backgrounds, but having everyone working together around the table and actively engaged was a significant ingredient in what made this Alliance different – and effective. The results have benefitted everyone involved, none more so than children in the countries which have seen improved access to vaccines and support.
Part of the motivation for creating Gavi was to provide children in low-income countries with access to vaccines as they were becoming available to children in wealthy countries. Particularly in the spotlight were vaccines to prevent rotavirusRotavirus
Rotavirus can cause inflammation of the stomach and intestines – and it’s the leading cause of deadly diarrhoea in children, which kills more than 500,000 children under five every year. Unlike other types of diarrhoea, improving hygiene does not prevent rotavirus infection, and it can’t be cured by antibiotics and other drugs – which makes prevention essential. The rotavirus vaccine was the first test of Gavi’s efforts to shorten the delay between vaccines being introduced in wealthy countries and in low-income countries. In 2007, the Alliance opened a funding window for rotavirus vaccines in Europe and Latin America – just one year after the United States and other high-income countries introduced the vaccine. Two years later, WHO recommended universal rotavirus vaccination, and Gavi expanded its support worldwide. Since then, more than 100 million children in 45 Gavi-supported countries have been immunised against rotavirus, saving lives and saving money: rotavirus vaccination helps avoid the unnecessary and ineffective use of antibiotics often prescribed for this viral diarrhoeal disease., one of the leading causes of diarrhoeal disease; and pneumococcalPneumococcal conjugate
Pneumococcal disease is the leading cause of pneumonia, which kills more children every year than any other infectious disease. Pneumococcal conjugate vaccines (PCV) are expensive, highly complex vaccines that would normally reach children in the poorest countries 10–15 years later than children in the richest countries. To close this gap, the Alliance worked with donors and the World Bank to develop the Advance Market Commitment (AMC) for pneumococcal vaccines. Launched in 2009, this innovative financing mechanism gives lower-income countries access to vials of PCV in doses that are most appropriate to the countries’ needs, as soon as a year after they were first made available – at an affordable cost of less than 10% of the US market price. By the end of 2019, a total of 60 Gavi-supported countries (more than 80% of those eligible to do so) had introduced PCV into their routine immunisation programmes, protecting more than 183 million children against pneumococcal disease. disease, a primary cause of pneumonia, the biggest killer of children under five. These were being developed or had started to be used in wealthier countries, but their price put them beyond the reach of low-income countries. In the past, it could take two decades or even longer for new vaccines to become available to people in poorer countries. Gavi’s ambition was to speed up that process dramatically.

4. Early challenges
4. Early challenges
From humble beginnings, with just a handful of staff operating from a small basement room, one of the initial challenges was how to achieve its ambition of developing new vaccines and delivering existing ones at scale.
Read chapter 4
The goal from Day 1 was to have impact at scale; the challenge was how to achieve that while also building a new organisation. The Norwegian public health leader Tore Godal became the first Chief Executive Officer, charged with creating a system that could deliver results – meaning vaccines – as quickly as possible. There was no doubt that the needs were great, but how could a handful of staff, operating from a small basement room in a UNICEF building in Geneva, make such an audacious idea a reality? Where to begin? Despite the level of ambition and commitment, and significant demand from countries for support, resources were limited in the early days.
We started with five people for the first couple of years. The major difference was that we then invited countries to submit proposals … and then we had an independent committee that assessed those proposals.
Tore Godal, founding CEO, GAVI

This independent assessment helped to build trust with countries and led to a growing number of high-quality applications for support. There was no shortage of demand from eligible countries. An early challenge was how to deliver new vaccines along with existing ones at scale. Part of the motivation behind the new Alliance was the failure to get enough vaccines to children in lower-income countries. Addressing this required a huge effort to deliver the triple childhood vaccine against diphtheria, pertussis and tetanus (DTP), together with Hib and hepatitis B. The task was considerable, but so was the progress. From 2001, when the very first Gavi-supported doses of hepatitis B vaccine were administered in Mozambique, to 2004, half of eligible countries had introduced the vaccine with Gavi support.
The pharmaceutical industry was eager to play an active role within the new Alliance, according to Jacques-François Martin, a senior industry official who became the first President of The Vaccine Fund. It was soon evident that bringing industry to the table was the most effective way to both deliver existing vaccines and develop new ones.
How can you say that we as an international community do not have the possibility to overcome this problem, which is clearly not an economical one? It is a matter of vision. It is a matter of ambition. It is a matter of governance, of organising ourselves, but we clearly, all together, have the possibility to make the case.
Jacques-François Martin, former President, The Vaccine Fund

We could never have engaged – or had shareholder support to engage – on such a long-term level of investment and commitment if we hadn’t had a high degree of confidence that there would in fact be a marketplace.
Andrew Witty, former CEO, GlaxoSmithKline
Yes, money speaks, and the US$ 750 million investment for GAVI meant we could create a big enough market to produce vaccines and drive research into new vaccines. And they knew that vaccines would be bought and distributed across the world, which is why it all worked.
Gro Harlem Brundtland, former Director-General, WHO; founding Chair, GAVI Board
From two to one
When the Global Alliance for Vaccines & Immunization (GAVI) was born in January 2000, it had a twin: The Vaccine Fund. The initial thinking was that it would be better to separate fundraising from operations. That proved to be complex; as the scale of the work grew, it became clear that a single structure would be both simpler and more effective. In 2007, the two entities agreed to merge and in 2009 became the GAVI Alliance. This name and the related logo remained in place until 2014, when the name was changed to Gavi, the Vaccine Alliance.
When the decision was taken to bring these two complex and very different entities together, an experienced chair was needed to ensure the discussions stayed focussed. It was not a simple task.
It was decided that it would be good to amalgamate The Vaccine Fund and the GAVI Alliance. And I was asked to chair that process, which I have to say stretched my chairing powers. It was a very, very difficult and prolonged process because there were so many different interests. But eventually we got it done. And I think the new GAVI Alliance Board greatly benefited from being able to focus on getting vaccines to children.
Mary Robinson, former Chair, GAVI Alliance Board
Cutting hepatitis B infections in China – a lasting success
An early and urgent problem was how to help China reduce hepatitis B – an infectious disease that causes liver cancer and cirrhosis. In the early part of this century, around one third of all people infected with the virus were in China. Between 2002 and 2010, with Gavi support, China immunised more than 25 million newborns and children under five in some of the poorest parts of the country. By 2005, the evidence of progress was so clear that the government decided to include hepatitis B in its routine immunisation programme. By the time the programme finished, nine in ten newborns were protected. An impact study showed that 685,000 future deaths and close to 4 million chronic infections were prevented during the period of Gavi support.
It was clear from their applications that one of the top priorities for Gavi-supported countries was to introduce the newly developed five-in-one pentavalentPentavalent
This was an early challenge that has become an outstanding success story. Combining five different vaccines in a single vial, pentavalent vaccine protects children against five major diseases: diphtheria, tetanus, pertussis (whooping cough), hepatitis B and Haemophilus influenzae type b. When Gavi was created, the five-in-one pentavalent vaccine was used primarily in wealthier countries, while low-income countries would require three separate vaccines to provide the same protection. Today, pentavalent vaccine protects children in all Gavi-supported countries and is the foundation of their routine immunisation programmes. By the end of 2018, more than 467 million children had been immunised with Gavi-funded pentavalent vaccine. Protection against five diseases through only three shots – instead of the previous nine – delivers substantial efficiency and cost savings for countries. Over the past 20 years, Gavi has worked with industry partners to significantly reduce the cost of pentavalent vaccine while maximising coverage. vaccine to protect children against DTP as well as Hib and Hepatitis B. By delivering all five antigens in a single shot, more children would be protected against more diseases. In 2001, Kenya was the first Gavi-supported country to use this new vaccine.
By 2014, all 73 countries then eligible for Gavi support had introduced it into their routine immunisation programmes. An additional benefit of the combined vaccine was its impact on storage and transportation. The reduction in pressure on logistics systems and the “cold chain” (to maintain vaccines at the required temperature) led to valuable gains for countries, and later became a significant focus for Gavi as it invested in improving the functioning of the cold and supply chains.
5. New ways of raising funds
5. New ways of raising funds
How the sheer scale of operations led to an entirely new and sustainable way of raising long-term funding for global health.

Read chapter 5
As the Alliance gathered momentum, the scale at which it was now operating presented new challenges. Gavi donors, including many European governments, Canada, the United States and the Bill & Melinda Gates Foundation, had been very generous from the beginning, but to continue delivering at scale required sustainable funding to match this. In the early 2000s, creative people working in treasuries and finance ministries had already begun to look at the potential of using capital markets to leverage their development funding and accelerate progress towards achieving the Millennium Development Goals (MDGs).
This thinking led to the development of the International Finance Facility for Immunisation (IFFIm), launched in 2006 by the United Kingdom together with France, Italy, Spain and Sweden, and later joined by Norway, South Africa, the Netherlands, Australia and Brazil. The idea was to use legal guarantees of future funding over a decade or more to raise money on the bond markets that could be used almost immediately to pay for vaccines. These bonds have been a huge success – 80 million children were vaccinated before funds were received by donors to pay for the vaccines. To date, IFFIm has attracted more than US$ 6.6 billion in long-term commitments going through to 2037 and financed close to a fifth of Gavi programmes.
The International Finance Facility for Immunisation is a unique instrument which Gavi uses to access capital markets to raise money and frontload resources with the guarantee of governments, so we can save lives sooner and faster.
Ngozi Okonjo-Iweala, Chair, Gavi Board

IFFIm has been a hugely successful innovative financing tool for Gavi. The thinking behind it also led to further creative ideas and the birth of a second innovative financing solution that made the most of Gavi’s model. The Advance Market Commitment (AMC) for pneumococcal vaccines was developed to incentivise manufacturers to rapidly take a new vaccine from research to development, and bring it to market by providing guarantees of price and volume for the resulting product. The vaccine offers protection against pneumococcal disease – the leading cause of pneumonia in children. Thanks to this innovative approach, children in 60 Gavi-eligible countries have now received a vaccine that would otherwise have taken more than a decade to reach them. The cost for Gavi-eligible countries is around 2% of that in high-income markets.

6. Much more than a handout
6. Much more than a handout
A new model for sustainable development: how Gavi aims to put itself out of business – by putting the governments of lower-income countries in the driving seat and on a path to fully funding their own vaccine programmes.
Read chapter 6
From the very beginning, it was important for the success of this Alliance that supported countries were directly engaged, and that both governments and civil society were actively involved. Governments have always had a seat at the table in Gavi’s decision-making, as well as a vital stake in the outcome of the Alliance’s work. Eligible governments also put their own money on the table to help ensure the success of their vaccine programmes. The importance of sustainability for Gavi funding became clear in the early days. As a result, the Alliance put in place a resource mobilisation strategy for Gavi-eligible countries through a system of co-financing. All countries applying for new vaccine financing through Gavi for certain vaccines must fund part of the cost. Today, the amount each country pays varies according to its income per head.
As countries become wealthier, they gradually take on an increasing share of the cost of vaccines. To date, Gavi-supported countries have invested US$ 1.6 billion in this way and through self-funded vaccine programmes. This reinforces country ownership of the vaccine programme and leads to self-sufficiency. Country contributions gradually rise to 100% of the cost of vaccines, at which point the country stops receiving Gavi support and starts to fully fund its vaccine programmes.
Who is eligible for Gavi support?
Gavi’s role is to support the world’s lowest-income countries. That is defined as countries with less than a given level of gross national Income (GNI) per capita over the past three years. In Gavi’s first five years of operation (2000-2005), the threshold was set at US$ 1,000, and 74 countries were eligible to apply for support. The level is revised every year and is currently US$ 1,630.
Although the original vision was to save lives and prevent disease, as Gavi’s impact grew, the potential to reduce poverty also became clearer. WHO estimates that as many as 100 million people are pushed below the poverty line every year because of health care costs. By preventing illness in the first place, Gavi is saving millions of people from this fate. Studies by independent health economists show that for every US$ 1 invested in vaccination, there is a US$ 54 economic return, through people living longer, healthier lives. Over its first 20 years, Gavi-supported vaccines have helped to generate more than US$ 150 billion in economic benefits.
Routine or campaign?
Gavi was created to accelerate access and increase coverage by providing new and underused vaccines to lower-income countries. Routine immunisation is essential to ensure that all children are protected against a core group of diseases. In some instances, routine coverage is not enough; or it can be critical to get rapid population immunity, and campaigns are needed (for example, when outbreak-prone diseases strike – like yellow fever, meningitis and cholera). Campaigns can also be used when a new vaccine is introduced, for example typhoid vaccine, inactivated polio vaccineInactivated polio
Polio is close to becoming the second human disease ever to be eradicated from the world, after smallpox. Polio has no cure, so immunisation has been critical in driving down the number of cases. Since the start of the eradication effort in 1988, when more than 1,000 children a day were being paralysed by the virus, the total annual number of cases globally had dropped to just 33 by 2018. However, the oral polio vaccine contains a weakened live version of the virus, which in areas of low vaccination coverage can lead to cases of vaccine-derived polio. To reduce this risk and make eradication possible, the inactivated polio vaccine (IPV) is now being used also. IPV does not cause vaccine-derived polio but can help strengthen children’s immune system and protect them from polio too. By the end of 2017, Gavi had helped more than 75 million children to be vaccinated against polio with IPV. And by April 2019, all Gavi-supported countries had introduced the vaccine into their routine immunisation programmes. to provide enhanced protection against polio, or measlesMeasles, 2nd dose
Measles is a highly contagious and deadly viral disease which can be controlled very effectively through high vaccine coverage. In 1980, before widespread vaccination, measles caused an estimated 2.6 million deaths each year. Beginning in 2006, Gavi supported the vital second dose of measles vaccine; in 2013, that support expanded to include two doses of the combined measles-rubella vaccine (see “Measles-rubella”). Despite considerable success in introducing the measles vaccine to Gavi-supported countries and a dramatic reduction in the number of deaths, stagnating coverage rates have contributed to a recent significant increase in the number of measles cases and serious outbreaks in many parts of the world. In high- and low-income countries alike, complacency and misinformation have led to vaccine hesitancy – leaving too many children unprotected against measles. In 2018, after years of decline, the number of cases increased, and more than 140,000 people died from measles, most of them children under five years of age. Gavi supports measles vaccine campaigns, combined with inclusion in routine immunisation programmes, to help lower-income countries protect their children from outbreaks. To date, Gavi has helped protect more than 118 million children against measles through routine immunisation and more than 524 million through campaigns. vaccine to build immunity within communities. Gavi support is tailored to strengthen both routine immunisation and campaigns when needed. As of the end of 2018, Gavi has supported the immunisation of more than 960 million people through campaigns.
Getting vaccines to a country is only part of the story. Immunising children also means finding and identifying those who need protecting; hiring and training health workers; getting vaccines to health centres; and keeping them cool until they’re needed. In other words, building and maintaining an effective health system. So from the start, part of Gavi’s mission has involved supporting governments to invest in their health systems and provide better protection to their citizens.
Keeping it cool in the cold chain
The “cold chain” plays a vital role in immunisation, ensuring that vaccines are kept at the correct temperature at all times. In countries where access is difficult and populations are spread across vast regions, keeping vaccines cool can be a major challenge. Different circumstances require different technological solutions: solar-powered fridges where electricity supply is unreliable; portable vaccine carriers and cooling equipment where vaccines must be transported over long distances. Building upon systems that WHO and UNICEF helped countries establish, Gavi enables countries to buy, distribute and maintain the equipment they need to ensure that there are sufficient supplies of vaccines to reach the people who need them. New technologies are more efficient and more sustainable, requiring less electric power and providing savings over the longer term, as well as a smaller carbon footprint.
7. Old diseases, new vaccines
7. Old diseases, new vaccines
Despite the progress Gavi was making, there was an urgent need to deliver powerful new vaccines to protect against some of the biggest killers of children.

Read chapter 7
The biggest killers of children are some of the oldest diseases around: diarrhoea and pneumonia. In the years leading up to Gavi’s birth, intense research and development work was being done on vaccines to prevent two of the main causes of these deaths: rotavirus and pneumococcal disease. While the top priority for countries and for the newly formed Alliance was to increase the availability and use of existing and underused vaccines, the ambition of all involved was to go much further. As well as wanting to ensure that children everywhere had access to the “basic” childhood vaccine – the five-in-one pentavalent – the Alliance was also focussed on the development and introduction of these new vaccines. By 2008, that vision had become a reality: through UNICEF, the first doses of Gavi-supported rotavirus vaccine, which prevents the deadliest form of diarrhoeal disease in young children, were purchased and introduced into routine immunisation systems. The following year, it was joined by pneumococcal conjugate vaccine, which prevents the primary cause of childhood pneumonia.
How it works in countries
Gavi does not have distinct offices or employ staff directly in countries; instead, the Alliance financially supports countries and works through partners who are active on the ground providing technical assistance. This often includes UNICEF and WHO, as well as national and international civil society partners. These Alliance partners are responsible for day-to-day engagement and management of Gavi-supported programmes.
One of the main goals of the new Alliance was to reduce the time taken between a new vaccine appearing in wealthy countries and being made available in lower-income countries. These two new vaccines were the first tests of this approach. Rotavirus was first offered to Gavi-eligible countries in Europe and Latin America just one year after it was introduced in the United States and other wealthy countries. This was real-world validation that it was possible to make new vaccines available almost simultaneously to children in the richest and poorest parts of the world. In 2009, Gavi started to offer support for the vaccine to all eligible countries. So far, more than 100 million children in 47 countries have been protected with rotavirus vaccine.
Pneumococcal vaccines can be complex to develop and manufacture. Similar vaccines have previously taken as long as 20 years to reach low-income countries. Thanks to guarantees of price and volume under the Advance Market Commitment (AMC) for pneumococcal vaccines, two manufacturers have already committed to supply 1.65 billion doses of appropriate vaccines through 2027 at affordable prices for Gavi-eligible countries. This alone will save more than 700,000 lives.
Most of the children who become sick and die from pneumonia are in low-income countries, and yet these countries have the fewest resources to protect them and had been among the last to get pneumococcal vaccines. Because of the Vaccine Alliance, this imbalance was finally being challenged. Since 2009, as many as 60 Gavi-eligible countries have introduced pneumococcal vaccines into their routine programmes – more than 4 out of every 5 eligible countries. Over 183 million children have been protected against this deadly disease. As well as being the main cause of childhood pneumonia, which kills more children each year than any other disease, pneumococcal disease can also cause meningitis and other life-changing infections. As a result of support from Gavi donors, the proportion of children protected with pneumococcal vaccine in low-income countries is now higher than in wealthier countries. According to the latest data, coverage rates in Gavi-supported countries reached 48% in 2018, compared to a global average of 47%. The availability of these relatively expensive vaccines in middle-income countries remains a challenge.
Emergency stockpiles
With some diseases, the name alone is enough to strike fear. CholeraOral cholera
Cholera is an acute intestinal infection caused by contaminated food or water. The disease affects both children and adults, and if untreated can quickly lead to severe dehydration and death within hours. Cholera kills somewhere between 21,000 and 143,000 people a year, affecting the most vulnerable populations – in slums, in rural areas and among displaced groups. Outbreaks are a serious risk during conflicts or following natural disasters where there is little access to clean water and sanitation, such as in Yemen and among the Rohingya refugee population in Bangladesh. After the 2010 Haiti earthquake, following which more than 8,000 people died of cholera, a global stockpile of the oral vaccine was created in 2013. Between 2014 and 2018, Gavi contributed more than US$ 110 million to the stockpile – which has been accessed 76 times by 24 countries, distributing more than 35 million doses of oral cholera vaccine., yellow feverYellow fever
This was one of the first vaccines supported by Gavi for use in campaigns (as well as routine immunisation). Yellow fever is an epidemic-prone viral haemorrhagic disease spread by mosquitoes. It can kill as many as one in two severely affected people. Rapid urbanisation and the resulting concentration of populations increase the potential for outbreaks and the spread of the disease, especially in Africa. Gavi has supported campaigns in 14 countries to protect more than 130 million people against the disease and has averted more than 1 million deaths. Today, Gavi supports preventive campaigns as well as routine immunisation in endemic countries, together with a global stockpile for use in emergency outbreaks., typhoidTyphoid conjugate
The typhoid conjugate vaccine is a revolutionary new means to prevent typhoid fever, which kills more than 128,000 people a year, mainly in sub-Saharan Africa and South Asia. Usually transmitted through contaminated food or water, typhoid can spread easily in places with poor water and sanitation systems. The vaccine is more critical than ever, as typhoid is increasingly resistant to drug treatments, a global problem which is threatening our ability to treat a range of potentially fatal infections. Without treatment, typhoid kills up to 30% of those infected. Previous typhoid vaccines only provided short-term protection and were ineffective in children younger than two years. This is one reason why, in 2008, Gavi had identified typhoid conjugate vaccine as a priority, because it can provide longer-term protection and can be effective in children as young as six months. When a safe and effective vaccine finally became available in 2017, Gavi approved US$ 85 million to support its introduction into routine immunisation programmes, the first being Pakistan in November 2019. High routine immunisation coverage with this powerful new typhoid conjugate vaccine can play an important role in controlling this deadly disease, and in helping the global community understand its impact on antimicrobial drug resistance. – these are plagues that have been known to humankind for many years. Today, EbolaEbola
Between 2014 and 2016, the world’s worst-ever Ebola epidemic devastated three countries in West Africa. With no vaccine and no cure, it was able to spread to major cities, infecting more than 28,000 people and killing more than 11,000 of them. In order to end the outbreak and prevent future ones, Gavi created a market for an Ebola vaccine through a unique agreement with pharmaceutical company Merck. This enabled a continuously replenished stockpile of 300,000 doses of experimental vaccine, which has since been used in outbreaks in the Democratic Republic of the Congo (DRC) to protect more than 250,000 people through a ring vaccination strategy – where rings of people around each infected person, such as friends and family, are vaccinated to prevent the further spread of the virus. In late 2019, Merck’s Ervebo® became the first Ebola vaccine to receive European Commission approval, WHO prequalification and FDA approval. Now Gavi is working with manufacturers and Alliance partners to create the first global Ebola stockpile and explore its use in prevention. has been added to that list of terrifying names. When one of these diseases strikes, rapid reaction is essential. That is why Gavi now funds emergency stockpiles for cholera, meningococcal meningitis and yellow fever. Eligible countries have access to the stockpile free of charge to help speed up the response, and they can also request funding to support the operational costs of campaigns. Non-Gavi countries can also use vaccines from the stockpile but are required to refund the cost. The Alliance has also just established an Ebola vaccine stockpile to help respond to and prevent outbreaks.
Although Gavi’s mission is global, in some cases diseases are concentrated in specific geographic areas, where they can do great damage. Meningococcal meningitis A is one example. For years, this disease had been causing regular and devastating outbreaks in the “meningitis belt” region stretching from east to west across a wide band of North and Central Africa. The Meningitis Vaccine Project was set up to develop a low-cost, targeted vaccine to prevent this specific strain of meningococcal meningitis and stop yearly outbreaks of the disease. In 2010, Gavi supported the introduction of the new vaccine for use in campaigns to reduce the terrible impact of this disease.
Because of this, more than 300 million children and young adults in 22 countries have been protected against meningococcal meningitis A; as a result, the number of outbreaks has dropped substantially. Since 2016, Gavi has also supported the meningococcal meningitis AMeningitis A
Africa’s “meningitis belt” stretches from Senegal in the west to Ethiopia in the east, with about 500 million people at risk of meningococcal meningitis, which can kill within hours – 1 in 10 die even with antibiotics. Since 2010, Gavi-supported meningococcal A vaccine campaigns have reached more than 296 million children and young adults in 22 countries with the MenAfriVac® vaccine. This was the first vaccine developed specifically for Africa, and crucially can be kept at temperatures of up to 40°C for 4 days, which makes it easier to deliver to remote places that lack refrigeration. The number of recorded epidemics has fallen to the lowest-ever level. While campaigns have been highly successful, routine immunisation is key to reducing the disease burden over the longer term. Gavi started supporting routine immunisation with meningitis A vaccine in 2016; by the end of 2018, over nine million children had been protected in this way. vaccine in routine immunisation in affected countries, although this uptake has progressed more slowly.

8. Building and rebuilding confidence
8. Building and rebuilding confidence
Now operating at scale, the extent of Gavi’s impact established the Alliance as an important global health player. Even at a time when international economic confidence was at a low, donor governments were ready to double their financial support of Gavi’s mission.
Read chapter 8
The end of Gavi’s first decade came with renewed financial challenges, following the banking collapse of 2008 and resulting intense pressure on donor governments. In 2011, the first Gavi Donor Pledging Conference was co-hosted in London by the Governments of the United Kingdom and Liberia, and the Gates Foundation, under the headline “Four hours to save four million lives.” Governments more than doubled their previous commitments, and new government and corporate donors made additional financial commitments.
Donors, who pledged US$ 4.3 billion, considerably exceeded the target and underlined their commitment to funding immunisation despite pressures on their own finances. Lower-income country governments also committed to maintain or increase the co-financing of their vaccine programmes, and manufacturers offered lower prices on several critical vaccines. The renewed financial support came at an important moment for Gavi: a record 50 countries had applied for vaccine funding – nearly double the previous record.
Here is what the co-hosts said at the 2011 Pledging Conference:
Gavi was one of the very top performers in our root-and-branch review of the agencies that deliver British aid, because it demonstrates tangible results.
David Cameron, former Prime Minister, United Kingdom
Today is an important moment in our collective commitment to protecting children in developing countries from disease. But every 20 seconds, a child still dies of a vaccine-preventable disease. There’s more work to be done.
Ellen Johnson Sirleaf, former President, Liberia
Together we must do more to ensure that all children – no matter where they live – have equal access to life-saving vaccines.
Bill Gates, Co-Chair, Bill & Melinda Gates Foundation
9. Helping markets to work better
9. Helping markets to work better
It wasn’t just donor governments that were noticing Gavi’s impact. Vaccine manufacturers were seeing the value of affordable, high-volume markets in lower-income countries. As a result, Gavi was helping to reach more children by creating healthier and more competitive vaccines markets.

Read chapter 9
One of the reasons Gavi was created was to address a major market failure. Part of its ongoing mission is to help make markets work better for life-saving vaccines and the people who need them. As the Alliance has grown, this part of its work has also expanded and become more complex. In the past, the challenge for manufacturers was how to balance investment and information. Developing and producing a vaccine takes serious amounts of capital investment, which is only possible with some guarantee that a market will exist for the final product. Before Gavi started working in this area, it was much harder for manufacturers to find out which vaccines were most wanted, and at what price. Today, Gavi works with both manufacturers and countries to improve the flow of information so that countries have a better idea of what is in the pipeline and producers know what the acceptable price range will be.
In addition to helping bridge the information gap, part of the challenge was to find ways to help the vaccine market shift its vision for low-income countries from selling its products at high prices in low volume to building a high-volume market that enables prices to be set far lower. In the past, low-income countries appeared on the periphery of manufacturers’ plans as “rest of world,” if they appeared at all. Today, thanks to Gavi, vaccine companies aim many of their products directly at this market. This shift was achieved in part by providing volume guarantees so that manufacturers could make the large up-front investments, knowing there would be a market waiting for their products.
At the same time, Gavi worked to encourage manufacturers in low-income countries to develop and export new products. Guaranteed prices in hard currencies enabled these companies to invest in increasing their production lines, generating greater competition in vaccine markets and providing a wider choice of products for Gavi-eligible countries. Many new manufacturers from lower-income countries have now entered vaccine markets, helping to improve supply and encourage healthy competition. When Gavi was launched, only one of the five vaccine manufacturers serving these markets with quality, pre-qualified products was in a lower-income country. Today, there are as many as 17 manufacturers, the majority in lower-income countries.
By understanding the planning processes of countries and the requirements and time horizons of manufacturers, the Alliance transformed vaccine markets, helping to ensure that they work for the benefit of people in low-income countries. This also enables donors to achieve maximum impact through their investment in Gavi’s work.
The important thing is that Gavi has gotten confidence in the way it works and what it does. It's important to industry to know that if there are new vaccines for developing countries, there will be an organisation that will help get them distributed; confidence among the donors that the money is well spent; and that if there is misuse, that countries will pay that back. And, of course, confidence among countries that after almost 20 years of having a reliable supply of vaccines, people can see this as something that can be used routinely going forward.
Seth Berkley, former CEO, Gavi

As vaccine markets developed and became more complex, it was also apparent that markets for other vaccine-related products were not working optimally. Given its success with vaccine markets, Gavi realised that if it applied a similar model to cold-chain equipment markets, it could also potentially open new opportunities for manufacturers and for countries to get better, more efficient equipment. Gavi began working actively to encourage companies to develop new products and at the same time helped countries to identify and buy the equipment they needed at affordable prices. By identifying gaps in the market for sustainable and efficient equipment, the Alliance is now helping countries to strengthen their cold chains and replace outdated equipment. This is also helping to protect vaccines, maximise efficiency and minimise wastage. At the launch of this effort in 2015, there were 10 products to choose from. Today, there are more than 74 ice-lined refrigerators and solar direct drive devices available, as well as innovations in remote temperature monitoring, freeze-free carriers and other technologies.
The polio endgame
The ultimate aim of any vaccination programme is to prevent a disease entirely. This has only been done with one human disease – with the eradication of smallpox. The Global Polio Eradication Initiative, of which Gavi is a part, has made huge progress, reducing the number of polio cases by more than 99%; but the disease clings on tenaciously in a few pockets. Gavi is an active part of the polio eradication effort and has supported the inactivated (and injectable) polio vaccine in all Gavi-supported countries. This vaccine will continue to protect children even after this terrible disease has been eradicated.

10. New tools, new approaches
10. New tools, new approaches
Gavi wasn’t just a new idea; it encompassed a novel way of thinking, of solving problems. That included the use of cutting-edge technology to overcome global health obstacles.
Read chapter 10
When Gavi was first created, its innovative model broke the global health mould. Since then, innovation has been essential. From the earliest years, the Vaccine Alliance has worked to find new and different ways of working, using novel partnerships, financing, data and technology to break down barriers and deliver new and existing vaccines to the people who need them. From championing the five-in-one pentavalent vaccine and a groundbreaking Ebola vaccine to investing in cold-chain technology, data management and the use of drones for delivery, Gavi continues to seek out new solutions and innovative approaches.
Vaccine Vial Monitors keep vaccines safe and cut waste
Vaccines are only effective if they are kept within a certain temperature range. The challenge is how to know when a vaccine has been out of the fridge too long. This is especially critical in hot climates where refrigeration is weak and electricity erratic. The solution is vaccine vial monitors (VVMs) – temperature-sensitive labels attached to each vial of vaccine which indicate temperature exposure over time to ensure the vaccine is still safe and effective to use. An easily identifiable change in colour shows when the vaccine has been exposed to higher ambient temperatures and can no longer be used. The monitors also help to reduce waste by identifying which vaccines in any batch are still usable and which must be discarded.
Such innovations came out of necessity. For example, it was not enough to get vaccines to people; it had to be done safely. Injectable vaccinations can carry the risk of spreading infections if needles are dirty or reused. But Gavi’s support of a programme to accelerate the adoption of auto-disable syringes, which can only be used once, together with the adoption of new standards for safe injections in lower-income countries, has helped reduce this risk. Similarly, the safety of vaccines can be undermined if they are not kept at the correct temperatures. Gavi’s support of vaccine vial monitors, small heat-sensitive stickers that are now placed on every vial, has helped ensure that vaccines are only used if they have been kept within the correct temperature range. These are all examples of how Gavi, as a learning organisation, is constantly testing the limits of what is possible, seeking new approaches to the challenges it faces and adapting accordingly.
Auto-disable syringes: double the ways to prevent disease
An early success for the Vaccine Alliance was the introduction and support of auto-disable syringes, which can only be used once and so reduce the risk of spreading infection through dirty or reused needles. In 2000, it was estimated that almost two in every five health care-related injections globally were delivered with reused or inadequately sterilised syringes, resulting in millions of cases of hepatitis B, hepatitis C and potentially human immunodeficiency virus (HIV). By supporting and promoting the use of single-use auto-disable syringes, Gavi has helped to dramatically reduce infections as a result of immunisation.

Vaccines are remarkable in that they produce the world's most precious resource: they save children's lives. And those children grow up to be teachers, they grow up to be nurses, they grow up to be leaders. And that in effect is the world's most precious resource. In the end, vaccines are about not only innovation, and power, but they're magical. And what Gavi does is surround itself with the magic and the miracle of vaccines.
Bill Roedy, Gavi Envoy; former Vice Chair, Gavi Board
11. Making the system work better – and for everyone
11. Making the system work better – and for everyone
As progress was made in boosting coverage and introducing new vaccines in countries, the focus began to shift to strengthening health systems in order to reach clusters of people who were still missing out.

Read chapter 11
The scale at which Gavi was operating, its successes in helping to shape vaccine markets and its impact on disease burden, had earned it widespread recognition as a major player on the global health stage. But even though it had made huge strides in helping countries to purchase and introduce new and underused vaccines, it was clear that still more was needed. One of the reasons so many children were not being vaccinated was the weakness of many health systems and their lack of resources. Grants and other support were developed to enable countries to invest in their immunisation systems and help boost vaccine coverage.
I think the magic of Gavi is that we don’t just work on vaccines. People say, ‘Oh, you’re a vertical initiative.’ I don’t see us as a vertical initiative. First of all, vaccines don’t deliver themselves, so we need to have adequate health systems, adequate supply chains and data systems, and surveillance and a cold chain.
Seth Berkley, former CEO, Gavi
Private sector collaboration and delivery
As well as working closely with pharmaceutical companies, Gavi also collaborates with many other private sector partners. One great example of how effectively this works is the partnership with Zipline. When a health worker needs urgent supplies, or roads are flooded or impassable, how do you deliver the vaccines? The answer in a growing number of places is to use a drone. In 2016, the Government of Rwanda partnered with the California-based technology company Zipline, Gavi and the international delivery company UPS to explore the potential of delivering health products by autonomous drone. Many parts of the country are too mountainous for a drone to land, so Zipline experimented with a system that drops precious supplies by parachute to health workers and alerts them via text message to collect the package. In 2019, also with support from Gavi and UPS, Zipline and the Government of Ghana launched a second nationwide network aimed at serving up to 2,000 health centres and 12 million people.
A lot of times, a vaccination worker doesn’t know exactly how many kids they’re going to need to vaccinate … so they have to bring extra, and they might end up throwing that vaccine out at the end of the day. Zipline makes it possible to totally change the way that model works, so now a health worker can go out to a village and bring nothing, and then count and say, 'I need X number of this vaccine and Y number of that vaccine,' place an order and receive exactly what they need – no more, no less.
Keller Rinaudo, CEO, Zipline
This has played an important role in helping to increase the proportion of children reached with basic immunisation in Gavi-supported countries in the past two decades from just under 60% to over 80%. This in turn made a major contribution to reducing childhood mortality by half and the number of children infected with debilitating diseases by 70% over the same period. This increase in the proportion of children protected is a remarkable accomplishment, especially as populations have increased rapidly over the same period. But despite this progress, clusters of inequity persist. Even when national immunisation coverage increases in countries, this can sometimes mask very low vaccination rates at the sub-national level. As a result, 10.4 million children in Gavi-supported countries still aren’t receiving any routine vaccinations.
Tales from a health centre in Cox’s Bazar, Bangladesh
Shabnoor and Sonia are community health workers, providing vaccines and other health services to the largely migrant population in the camps of Cox’s Bazar, Bangladesh. Shabnoor, who was born in one of the camps, goes from door to door to identify unvaccinated children and give parents more information about vaccines. She said that over time, parents have come to trust her and her colleagues and now want to vaccinate their children. “My job is to ensure that everyone understands why vaccines are so important,” she said. “The relationship of trust is essential, in particular for community health workers.” Sonia provides vaccines in a UNICEF primary health care centre. She said she became a health worker because she wanted to put her skills to good use. “Vaccines help prevent diseases, and they save a lot of lives,” she said. “I became a health worker to help people stay healthy and find peace.”
These “zero-dose children” are among the hardest to reach in any country. Two-thirds live below the poverty line; some are in remote rural areas, but many are found in major cities – in urban slums or temporary settlements. They are often not registered with health centres, or with any other public services. They and their families may belong to marginalised communities with limited access to services or information.
Gavi works with governments and with civil society to help provide all children with the benefits of immunisation. To reach these zero-dose children, Gavi is accelerating its efforts, investing in training for health workers and improved logistics, and working to improve data collection and management and health leadership. This includes everything from using artificial intelligence technology to help fill the gaps in poor data systems and identify where communities are still missing out, to working with countries to help them prioritise and make more efficient use of their resources so that they target areas where clusters of zero-dose children are living.
The essential role of civil society
Civil society is a vital part of the Vaccine Alliance, supporting national and local vaccination efforts in every Gavi-eligible country and playing an active role on the Gavi Board. A wide range of civil society organisations work as part of the Alliance to support the introduction of new vaccines and help ensure that people everywhere receive the benefits of vaccines. Civil society voices bring different and important perspectives to all operational and policy issues discussed by the Board.
This is a critical part of Gavi’s mission. Health systems are complex and require many people with different backgrounds and skills to work effectively. When the system does work well, the beneficiaries are children and their families – including the poorest and those previously unreached with vaccines. Gavi works to ensure that vaccines reach as many children and young people as possible, regardless of gender, wealth or social status.
By protecting children with vaccines, health workers are helping to build the foundations of lifelong health care and strengthening ties with local communities. Governments around the world have made commitments to deliver affordable health care to every citizen (known as Universal Health Coverage), and to reach the ambitious targets of the 2030 Agenda for Sustainable Development. This will require continued investment in delivering primary health care to all – from antenatal care for women, through a child’s birth and protection with vaccines, to ongoing care throughout childhood and adulthood.
Despite two decades of progress in reaching a growing number of children with vaccines, combined with global poverty reduction, those who remain unreached are often in perilous situations. An increasing proportion of the countries which still need Gavi’s support are fragile states, affected by severe challenges including conflict, the climate emergency and human migration. The work that remains to be done is therefore harder in many ways than what has already been achieved. New approaches are needed, such as working more directly in specific regions of a country and with under-served communities. Conversely, it is becoming clear that a high and rising percentage of children around the world who have not been fully immunised are in middle-income countries. This poses a challenge to the global community, including to Gavi and its original mission to serve lower-income countries.

12. Focussing on women and girls
12. Focussing on women and girls
How Gavi is stepping up its work to ensure that girls and boys receive vaccines equally in all countries, and how it is breaking down the gender-related barriers that can prevent children of all genders from missing out.
Read chapter 12
As Gavi continued to make progress, it became clear that barriers to immunisation were not just economic or physical, but also sometimes based on gender. At a global level, girls and boys are vaccinated equally, but in some countries there is a gender imbalance so that more boys are protected with vaccines. Immunisation is not gender-neutral in its impact. In Gavi-supported countries, women are the main caregivers, so vaccination strategies must ensure they are actively engaged and, for example, that vaccinators knock on doors when there is most likely to be someone at home to let them in to vaccinate children. Gavi works hard to ensure that all genders are equally protected with vaccines.
But access isn’t the only gender-related issue. Some pathogens affect women more than men, such as human papillomavirus (HPV)Human papillomavirus (HPV)
Globally, one woman dies of cervical cancer every two minutes. With 311,000 deaths a year, it now kills more women than pregnancy complications and childbirth combined. The human papillomavirus (HPV) vaccine can prevent up to 90% of all cervical cancer cases, but when it was first launched in 2006, it cost more than US$ 100 per dose – putting it far beyond the reach of most women in lower-income countries, where 90% of cervical cancer deaths occur. Since Gavi has supported it, the cost of the HPV vaccine has been reduced to less than US$ 5 per dose for lower-income countries, a record-low price. Vaccination is especially critical in these countries, as women have limited access to screening or treatment. Since 2013, with Gavi support 3.9 million girls and young women have been protected against HPV., which is the cause of almost all cervical cancer cases. In countries supported by Gavi, where screening and treatment is not widely available to most women, this has become a leading cause of cancer deaths among women, now killing more women than pregnancy complications and childbirth combined. This growing problem led Gavi to start providing support for the HPV vaccine. First introduced in 2013 with Gavi support, this vaccine was unusual, not just because it prevented cancer, but also because its effectiveness was dependent on immunising young women and girls. This meant that the vaccine could not be introduced into routine childhood vaccination programmes.
To address this, initially a series of HPV demonstration programmes was launched to test the feasibility and cost of vaccinating adolescent girls in low- and middle-income countries. These have been completed in 30 countries. There are now 27 countries which have introduced or been approved to include the vaccine as part of their national immunisation programmes, protecting nearly 4 million girls and young women. To date, 18 Gavi-supported countries have introduced HPV vaccine nationally, of which 5 countries – Malawi, Tanzania, Uganda, Zimbabwe and Zambia – carry amongst the top 10 highest cervical cancer burdens in the world. Countries can now also apply directly for support without the need for a demonstration programme. Support for this vaccine has been so popular among countries that surging demand has created supply challenges, but Gavi is committed to continue supporting countries to introduce the vaccine.
The HPV vaccine also represents a significant success for one part of Gavi’s market-shaping work. By working closely with countries and industry partners, the Alliance has been able to deliver the vaccine to countries at an affordable price, preventing infections and saving many lives.
13. The risks of global health insecurity
13. The risks of global health insecurity
Despite the landmark progress Gavi has made, global trends are threatening to increase the risk of outbreaks. How this is making Gavi’s ongoing work ever-more important in protecting not just vulnerable children, but the whole world from persistent and new threats to global health security.

Read chapter 13
Despite the progress the Alliance continues to make, one of the most worrying challenges is global health security. The world has become ever more interconnected. Every year, 1 billion people cross international borders, and the global number of people displaced has now exceeded 70 million. Disease outbreaks can develop faster and travel further than ever before. Emerging threats are not confined to one place or one country, so investing in health security must be a global priority.
Environmental, demographic and social challenges like urbanisation, the climate crisis, migration and fragile states increase pressure on human societies everywhere, and especially in the lower-income countries which Gavi supports. Recent unprecedented outbreaks, such as the emergence of Ebola in urban areas, the alarming upsurge of vaccine-derived poliovirus outbreaks in several African and Asian countries, and the resurgence of measles in under-immunised, mainly urban populations – as well as the alarming rise and spread of drug-resistant pathogens – demonstrate the ever-present risks of infectious disease. In all these cases, effective immunisation is the best way to prevent infections in the first place, and to protect both at-risk populations and ultimately everyone else.
Because of its role in disease prevention and the scale at which it operates, the Alliance has an increasingly important part to play in improving global health security. Whether investing in a new vaccine market and then supporting the development and testing of new vaccines against Ebola, finding the best way to prevent new disease outbreaks or through the expansion of routine immunisation systems and strengthening of primary health care, Gavi’s work now has a significant impact not just on the lives of individual children, but also in helping to make the world safer.

14. Looking to the future
14. Looking to the future
Gavi’s impact has far exceeded the original vision. It has not only helped protect more than three-quarters of a billion children, but also helped boost the economies of poor countries and make the world safer. Now it is looking to go even further.
Read the last chapter
At the youthful age of 20, the Alliance has dramatically increased immunisation rates in low-income countries. Since 2000, it has helped protect more than 760 million people from infectious diseases, a figure which rises to well over one billion when vaccine campaigns are included. This has saved more than 13 million lives and contributed US$ 150 billion in economic benefits in supported countries. These numbers and the extraordinary achievements they represent are far beyond the dreams of Gavi’s founders, but there is still much more to do and too many people who do not yet have access to the enormous benefits of immunisation. Gavi has delivered protection to a generation of children and has contributed to the economic development of countries in ways that were not even understood in the early years. The next-generation challenge for Gavi is to help identify, find and protect every child who has never been vaccinated and bring them into the routine health system, as well as the many others who are not fully protected against all vaccine-preventable diseases.
Ebola and a new vaccine
The outbreak of Ebola that struck Guinea, Liberia and Sierra Leone in 2014 was the largest ever, killing 11,310 people among more than 28,000 who were infected. The unprecedented number of cases, combined with the spread of disease in urban areas, prompted the global health community to come together and support the development of a new vaccine. Gavi played a pivotal role in this by committing up to US$ 300 million towards the procurement of a vaccine when one became available, effectively creating a market where previously there was none, providing manufacturers with the necessary incentive to develop new vaccines. While the first of these, Merck’s Ervebo® vaccine, went through the regulatory process, Gavi also provided operational funding for its compassionate use pending approval in the Democratic Republic of the Congo, where more than 270,000 people have now received the vaccine. Following the regulatory approval and WHO prequalification of Ervebo® in November 2019, Gavi will now fund a global emergency stockpile of 500,000 doses for future use.
Liberia has regained to a large extent the trust of people. However, that will only last if we can do more to rebuild the health care system, and we have a long way to go. … A sick nation cannot be a working nation.
Ellen Johnson Sirleaf, former President, Liberia
What Gavi has achieved over the years is enormous success in reaching children all over the world with all kinds of vaccines. That is something that we had hoped for, but never anticipated, but it really has occurred.
Carol Bellamy, former Executive Director, UNICEF; former Chair, Gavi Board
Simply put, Gavi’s overarching ambition is to put itself out of business. Already, 15 of the countries that were originally supported have become fully self-sufficient in funding their immunisation programmes, with more to follow. In the coming years, we will face new and growing challenges. Supporting countries and ensuring that even the most fragile nations can protect their children will be another challenge in the coming years. Gender-related barriers still exist in many societies – preventing parents from fully protecting their children and women from accessing the benefits of immunisation. Poverty and insecurity remain obstacles to progress in many lower-income countries. Reaching every child is at the heart of Gavi’s next five-year plan, helping to deliver vaccines to people who need them everywhere, regardless of their gender, ethnic or social identity.
Gavi stands ready to support much-needed new vaccines to protect against AIDS, tuberculosis and malaria – the three killer diseases which still do so much harm around the world. In fact, work has already started to introduce a vaccine against malaria. In addition, new vaccines are being supported as they are developed, to tackle infections such as respiratory syncytial virus (RSV), a significant cause of respiratory illness in infants, and to target other cancers and chronic diseases as they are better understood.
A gateway to health for all
Expanding the reach of childhood immunisation is one of the best and most cost-effective ways to achieve Universal Health Coverage, the idea that everyone, everywhere, has access to affordable, quality health care. Vaccines don’t deliver themselves. They require supply chains, infrastructure and cold-chain facilities, all of which are essential for a range of other health interventions. They also need trained health workers, transport, community outreach, data services and disease surveillance, which can help improve the detection of and response to disease outbreaks. When a community gets access to childhood immunisation, it is often not long before they also get access to a range of other health interventions, such as maternal and neonatal care, deworming and malaria prevention. So by improving the reach of immunisation, Gavi effectively acts like a platform on which stronger primary health care can be built, also helping to mitigate against threats to global health security and improve resilience to climate shocks.
However, despite the progress Gavi has made, in the coming years all this will become increasingly more difficult. Not just because the last to be reached are the hardest to reach, but also because formidable global trends, such as climate change, population growth, urbanisation, human migration and antimicrobial resistance, threaten to increase the risk of outbreaks. At the same time, as economies grow, we will see an increasing proportion of under-immunised children in countries that are not supported by Gavi, to the extent that by 2030 we expect 70% of them to be living in middle-income countries.
The vision is a world where everyone has a right to disease prevention and primary health care, a world where the risk of outbreaks is reduced while the resilience of every country to the health impacts of climate shock is dramatically increased. In light of the growing challenges, if Gavi is to realise this vision, it will need to do what it’s best at: collaborate. That means not only continuing to work with core Alliance partners, but also working more closely with governments of lower-income countries to help them strengthen their immunisation programmes. And by continuing to forge new partnerships with sister organisations like the Global Fund to Fight AIDS, Tuberculosis and Malaria, it can become even more effective and efficient.
Two decades ago, it would have been difficult to imagine just how far Gavi would come, what could be achieved and at what scale, from that original audacious vision. During that time, it has transformed itself as an organisation almost as much as it has the hundreds of millions of lives that it has helped protect. It set out to solve one global health problem, but along its journey encountered countless others, each time finding solutions as it went. And yet, that original mission remains central, with the Vaccine Alliance and all its members committed to keep working to provide the benefits of immunisation, no matter what new challenges it encounters, to help countries to build resilience and ensure that no one is left behind without the life-altering benefits of vaccines.

My vision and hope is that in the next 20 years, we will work ourselves out of a job. My hope is that 20 years from now, maybe we'll have only 10 countries we are working in. Success is when governments and countries take over their own programmes and run them fully.
Ngozi Okonjo-Iweala, Chair, Gavi Board
Gavi's work can be measured in many ways. Over 13 million lives have been saved. The vaccine manufacturers know that there's a market even in these developing countries, so now we have an innovation pipeline of new vaccines that people are working on, knowing that Gavi will be there to make sure they get to the children who need them.
Bill Gates, Co-Chair, Bill & Melinda Gates Foundation

Roll the credits
Editor-in-Chief
Duncan Graham-Rowe
Editor & writer
Iain Simpson
Project coordinator
Susann Kongstad
Writers
Priya Joi & Amanda Tschopp
Interview support
Isaac Griberg, Doreen Mackay,
Wambui Munge, Chioma Nwachukwu
Svetlomir Slavchev & Jeff Weintraub
Graphic concept & design
Hervé Montandon
Illustrations
Amandine Comte
Photo sourcing
Jacques Schmitz
Videography
Svetlomir Slavchev
Web development & design
Alister Bignell & Natasa Milovanovic
Media
Isaac Griberg
Distribution & social media content
Elinore Court, Isaac Griberg
& Wambui Munge
Additional support
Lubna Elmahdy & James Fulker
Director of publication
Pascal Barollier