
A preliminary assessment of COVAX’s impact in lower-income countries
Approximately 90% of COVAX-delivered COVID-19 doses have gone to lower-income economies. This represents the fastest and most complex global deployment of vaccines ever. But in terms of achieving equitable access during this pandemic, how successful has it been and where have its impacts been the greatest?
White Paper
May 2023
Contents
Coverage in “never-Gavi” countries
Disclaimer:
This document is published by Gavi, the Vaccine Alliance. The contents included is the result of a collaborative process managed by Gavi. The republication or usage of the content of this document of any kind without written permission is prohibited. Please contact media@gavi.org with any requests for use.
Share
Executive summary
COVAX was launched in April 2020 to ensure that people in all corners of the world get equitable access to COVID-19 vaccines. With its first deliveries commencing in January 2021, COVAX delivered nearly 1.9 billion doses of vaccine to people in 146 economies by the end of 2022.
Approximately 90% of these doses have gone to lower-income economies. This represents the fastest and most complex global deployment of vaccines ever. But in terms of achieving equitable access during this pandemic, how successful has it been and where have its impacts been the greatest?
This white paper, the first in a two-part series, aims to answer that question, by looking at COVAX’s impact in lower-income countries, those referred to as “Advance Market Commitment” participants. The second paper will focus on the ways in which high-income countries (HICs) and upper middle-income countries (UMICs) have benefitted from COVAX, while also helping it deliver on its mission, as self-financing participants.
Before COVID-19, no global agreement existed to make pandemic vaccines accessible to everyone, other than for influenza vaccines. Without one for COVID-19 vaccines, the fear was that we would see a repeat of what happened during the previous pandemic, H1N1 influenza, when wealthy countries monopolised vaccine supplies leaving virtually none for the rest of the world. COVAX was created to prevent this from happening again, as a partnership of four core organisations, in the midst of the worst global health crisis in a century.
The Coalition for Epidemic Preparedness Innovation (CEPI) supported vaccine research, development and manufacturing scale-up from the lab to the production facility. Gavi pooled procurement and incentivised manufacturing expansion to secure supply of safe and efficacious vaccines, while also supporting in-country delivery. UNICEF coordinated procurement and distribution across COVAX participants, and also supported in-country delivery. The World Health Organization (WHO) provided normative guidance on vaccine policies, safety, regulation and allocation, with PAHO handling vaccine procurement and distribution in the Americas. Thanks to this partnership, nearly three years later, COVAX is continuing to protect some of the most vulnerable people in the world from the ongoing pandemic.
Today, even as COVID-19 continues to spread, the threat of future pandemics is not only increasing, but thanks to global trends like climate change, population growth, urbanisation and human migration, could double in the coming decades. As global leaders discuss how we should prepare for and respond to future pandemics, gaining a better understanding of how COVID-19 solutions performed will be critical to ensuring we have even more effective solutions in place next time.
Indeed, we now have not just an opportunity but a responsibility to learn from this experience for future pandemics. This in turn will help ensure that solutions aimed at global equitable access to essential medical interventions are in place before disaster strikes, and that the people most at risk will get the protection they need faster and more efficiently. Drawing on analysis of COVAX’s impact during the first critical year of deliveries and beyond, this paper aims to provide valuable insights into how this might be achieved in the future, while providing a list of key learnings that could be deployed to shape future mechanisms.
COVAX’s objectives
The greatest impact of vaccines during a pandemic lies with rapidly protecting high-priority groups – those most likely to come into contact with a virus and those most vulnerable to severe illness or death – and then slowing the spread or effects of the disease by increasing coverage more broadly. With this in mind, COVAX was designed with the rapid protection of high-priority populations (as defined by WHO SAGE guidance1) as its number one priority. Its initial goal was to secure enough doses of COVID-19 vaccine so that participating governments could protect all health and social care workers, older people and vulnerable citizens. But how much is enough?
The proportion of a country’s population that is made up of high-priority groups can vary significantly, depending upon demographics, culture and wealth. However, according to the WHO’s Fair Allocation Framework, most countries should be able to protect their high-priority groups with doses sufficient to protect approximately 20% of their population.
Based on this guidance, COVAX’s initial target was to secure sufficient supply to provide that proportion free of charge to lower-income countries by the end of 2021 – a total of some 950 million doses. Doses would be made available through the Gavi COVAX Advance Market Commitment (AMC), an innovative financing mechanism largely funded by donor governments, to countries that could not afford them. For higher-income countries that could afford to pay for their own doses, up to 950 million doses were to be supplied to them as self-financing participants (SFPs). Up to an additional 100 million doses would also be made available to people who were effectively stateless or in humanitarian settings, via a Humanitarian Buffer.
By delivering up to 2 billion doses in total, COVAX’s initial aim was to provide enough for participating countries to protect all their high-priority citizens and support vaccination across humanitarian settings. Beyond this, part of its ongoing mission was to continue to secure doses, more than 4 billion, to help the 92 AMC-supported lower-income countries increase their coverage beyond high-risk groups as the epidemiology and recommendations became clearer.
In 2021, COVAX adopted a goal of helping countries to meet their national vaccination ambitions. While the WHO made a distinct call in the third quarter of 2021 for every country to protect 70% of its population, this was never adopted as a target by COVAX. In part, this was because of the younger demographic profile of many AMC countries, which would have meant that to reach the target, vaccinations would have been necessary among children and adolescents, which at the time was not a COVAX priority. While COVAX supported the ambition of WHO, it maintained its focus on supporting countries to achieve the targets that they had set for themselves based upon local contexts and demographics.
COVAX coverage
To protect the most people, COVAX sought to roll out vaccines to high-priority populations as rapidly as possible, with its first doses reaching people in lower-income countries in January 2021, just 39 days after high-income countries first started to make them available. Within 42 days of this global rollout, COVAX had delivered doses to 100 countries. However, in the months that followed further deliveries were interrupted by a series of well-documented delays. This meant that until August the pace of rollouts reduced dramatically, as a result of vaccine hoarding, export bans and other factors. This was compounded by the fact that global financing for the delivery of vaccines from other sources was not reaching countries. So even when COVAX supplies started to ramp up, following a proactive response by COVAX to secure donations and alternative suppliers, a lack of absorption capacity within countries risked creating further delays.
To help countries address critical funding gaps for delivery scale-up, COVAX provided time-sensitive, country needs-based funding in the form of COVID-19 Delivery Support (CDS), as well as convening and leading the COVID-19 Vaccine Delivery Partnership (CoVDP). By the end of 2021 it had delivered 830 million doses to lower-income countries. This represents about 88% of the 950 million target, which it hit a few weeks later in mid-January of 2022. In 2021, COVAX provided 82% of the doses received by low-income countries (LICs) as well as 80% of those going to countries in the WHO AFRO region.
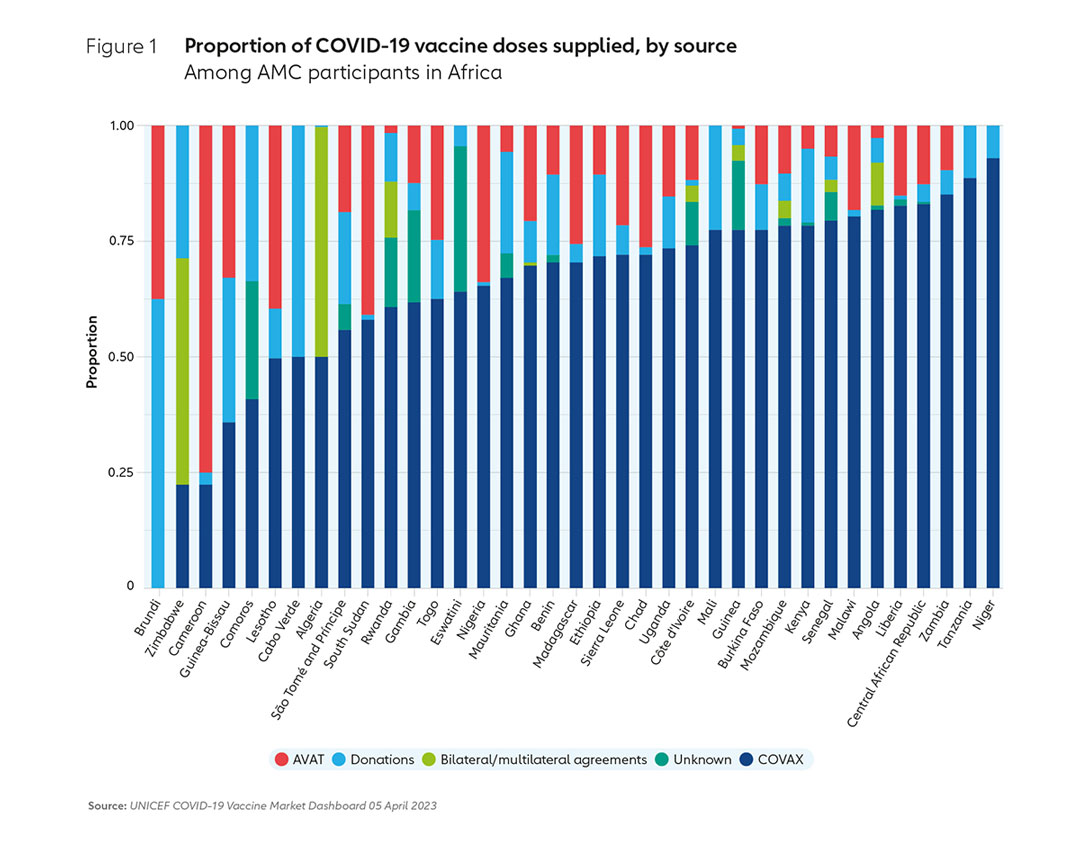
Following fresh resurgences after the emergence of Omicron, with more cases in 2022 than in the two years prior combined, the global supply constraints eased and deliveries continued to ramp up. By the end of 2022, COVAX had delivered 1.9 billion doses in total. As of mid-April 2023, this had risen to 1.95 billion doses. COVAX continued to be the main supplier to these countries, delivering approximately 73% of all doses supplied to LICs, and 69% to African AMC-supported countries by December 2022. As of mid-April 2023, COVAX had supplied 74% of all doses to LICs, and 69% to African AMC-supported countries. This suggests that COVAX continues to provide a lifeline to those countries that need it the most, those that would otherwise struggle to get access.
However, translating delivered doses into improved coverage has presented additional challenges. Progress was by no means uniform across the AMC-92 countries, with low-income countries in particular experiencing acute challenges in absorbing large volumes of doses once they started arriving. The Vaccine Alliance had been working in most of these countries for years, supporting routine immunisation and broader health system strengthening efforts. This included investments in cold chain infrastructure and other system aspects, along with funding and support for readiness before the arrival of COVID-19 vaccines via CDS funding. While this helped to build capacity that would be useful for years to come, for many LICs these investments did not come fast enough. Because of a lack of timely surge financing, challenges in getting the necessary human resources in place and the sheer scale of the task, large equity gaps remained.
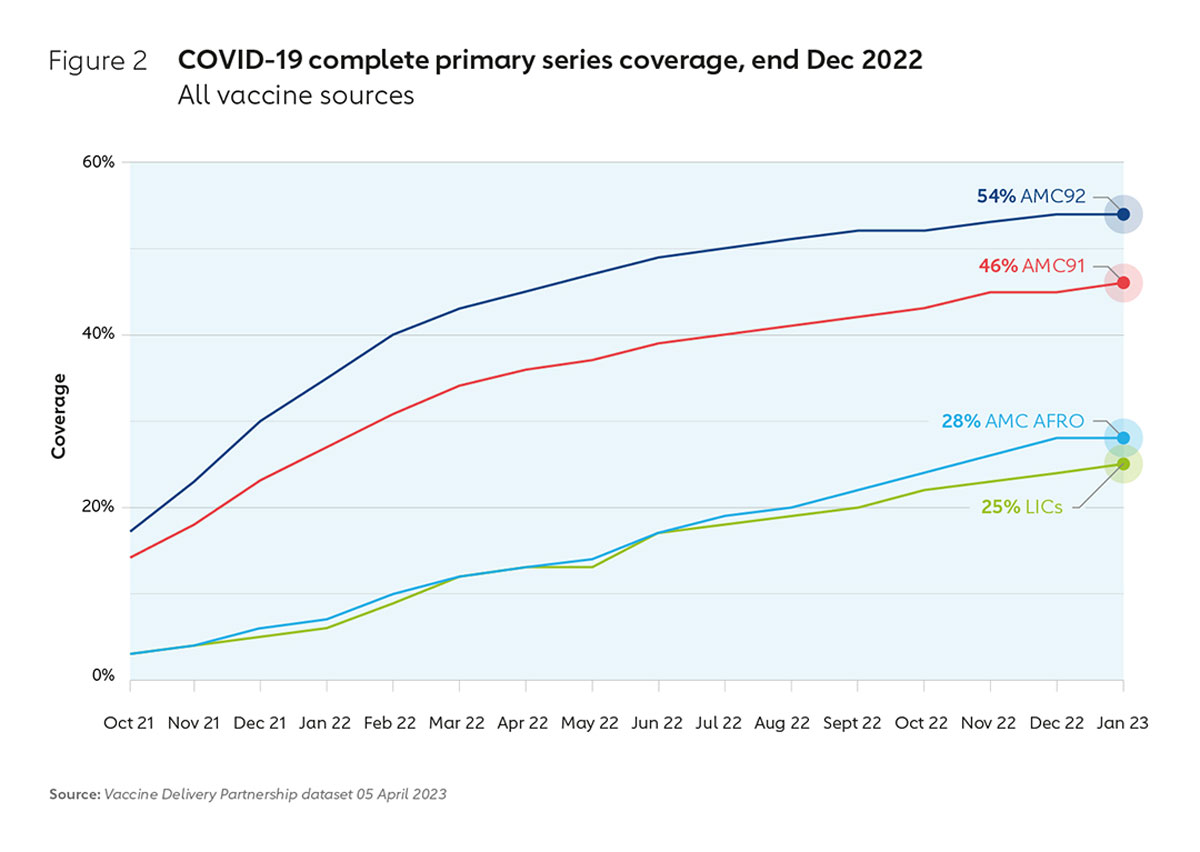
As a result, at the beginning of 2022, there were still 34 countries covered by the COVAX AMC that were below 10% COVID-19 vaccination coverage, with 28 of them in Africa. Since then, thanks to the incredible work of countries, with responsive support from COVAX through the CoVDP, 28 countries have moved past this milestone – with Cameroon, the Democratic Republic of the Congo, Gabon and Mali becoming some of the latest to do so. Thanks to targeted support and renewed political will, many countries in this group have more than doubled their coverage rates since January 2022, and some much higher – with countries like Côte d’Ivoire, Ethiopia, Tanzania and Zambia reaching 30% or more. And while efforts continue to close the remaining equity gaps, the fact that at the end of 2022 more than 50% of the populations covered by the COVAX AMC had received their full primary series, and over 80% of AMC economies were boosting their populations, is remarkable.
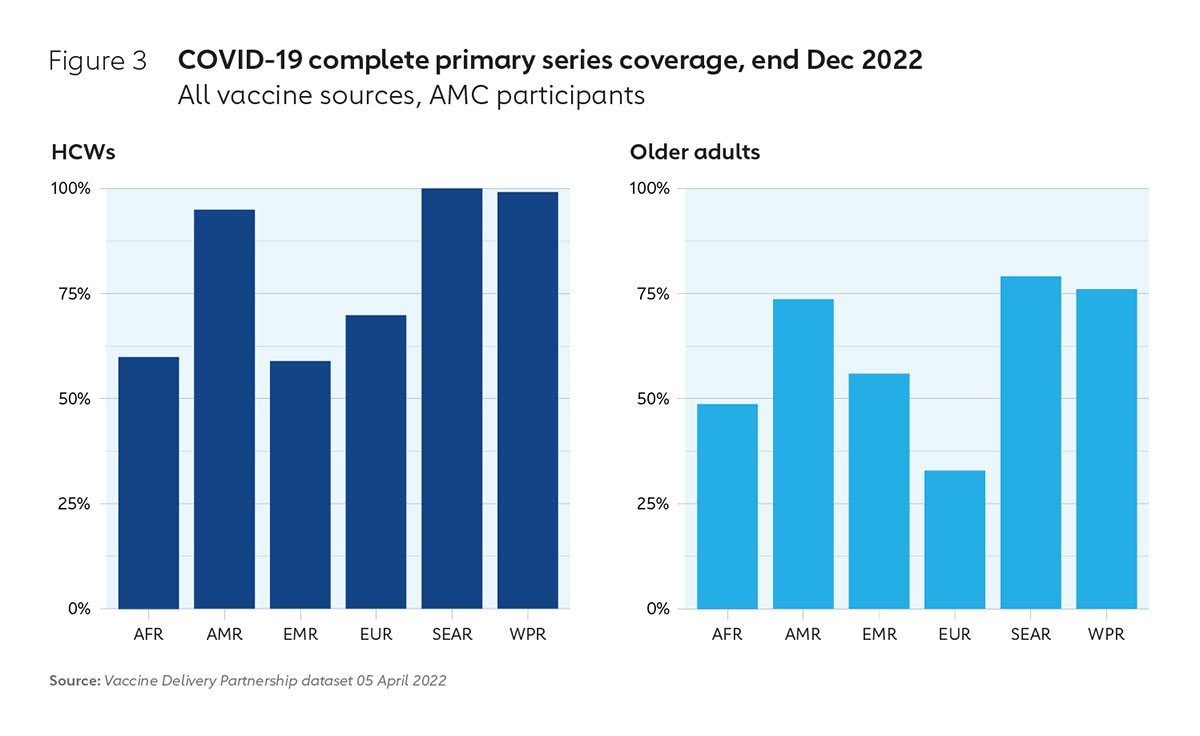
Providing doses to these countries through COVAX enabled AMC countries to reach 54% of their citizens with a complete primary vaccination series by the end of December 2022, higher than the 20% needed to protect those people most at risk such as health care workers and older people. As of December 2022, 81% of health care workers had been fully protected in AMC countries – more than current estimates in many high-income countries – and 67% of older people. In AMC countries in Africa, 60% of health care workers have now received a complete primary series and 49 % of older adults.
Box 1: India
Given India’s large population and the desire to ensure balanced support against the needs of other AMC participants, in December 2020 the Gavi Board endorsed plans to provide it with support, including approximately 240 million doses to be financed via the COVAX AMC. This volume of doses was always intended for India to supplement its own domestic vaccine production. These planned COVAX AMC doses were supported by a specific tech-transfer agreement, facilitated in part by the Bill & Melinda Gates Foundation (BMGF) and Gavi, between the Serum Institute of India (SII) and AstraZeneca to enable the rapid scale-up of manufacturing capacity, to benefit both COVAX and to serve India’s needs.
While India benefited from the first COVAX AMC doses delivered via SII in January 2021, this milestone was swiftly followed by an aggressive second COVID-19 wave which resulted in overwhelming domestic need in India. In view of this crisis, the Indian government imposed a de facto ban on vaccine exports beginning in April 2021. This resulted in a significant shortfall in planned COVAX shipments, throughout 2021.
Given that hundreds of millions of doses intended for COVAX were diverted to vaccinate and extend protection for the Indian population in 2021, indirect impacts may also warrant consideration. SII vaccines contributed significantly to India’s coverage gains that year, which saw more than 850 million people receive at least one dose, with 617 million receiving the complete primary series in 2021. They also enabled India to mount the world’s largest domestic COVID-19 vaccination campaign, helping to avert an estimated 3.6 million deaths in 2021 alone. Over 80% of all COVID-19 vaccinations in India in 2021 used the SII-AZ vaccine facilitated by Gavi for COVAX.
Coverage in “never-Gavi” countries
When considering impact, it is also important to bear in mind that a significant number of the 92 AMC countries supported by COVAX were in some ways at an increased risk of falling between the cracks without that support. Of these 35 countries, 12 were former Gavi-supported countries and all were classified as low- or lower middle-income. This meant that most of these countries were not only unable to afford to pay for COVID-19 vaccines themselves or enter bilateral contracts with manufacturers, but were also no longer receiving support from Gavi for their national immunisation programmes prior to the pandemic, and 23 of them had never received such support. Without COVAX they would have had no safety net at all.
As a core COVAX partner, this meant Gavi had to build new relationships and ways of working with many of these countries, and in the case of the 23 “Never-Gavi” countries, it had to do so from scratch. By the end of 2022, despite the challenges this posed, COVAX was able to help have a significant impact in these countries, supplying more than 35% of all doses they received and helping them to achieve 48% coverage with complete primary series. Furthermore, COVAX’s impact in these countries includes reaching most at-risk communities: among those countries that have reported data, 74% of health care workers and 56% of older people have been vaccinated.
Lives saved by COVAX
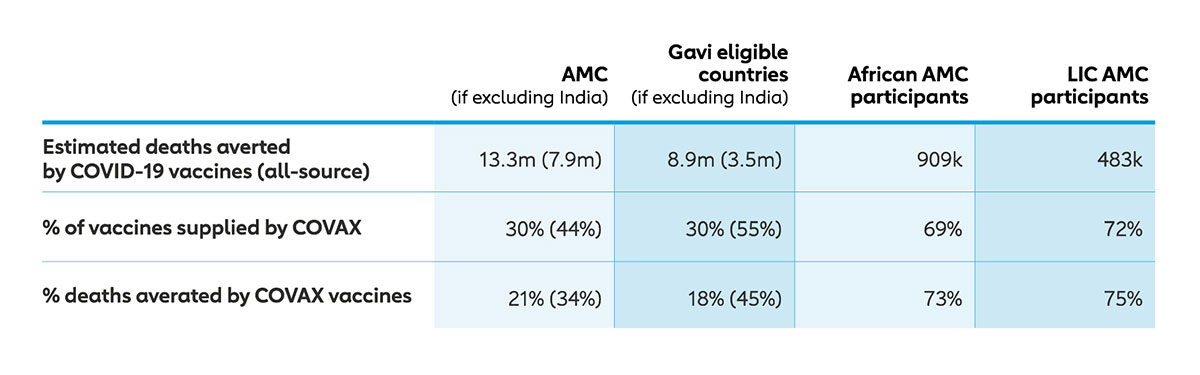
Independent modelling by Imperial College London, commissioned by the COVAX Facility, found that COVID-19 vaccinations averted 6.5 million deaths in AMC countries by late 2021. With 24% of doses received by these countries coming through COVAX, around 857,000 of these deaths averted – or 13% – were attributable to COVAX. Arguably more deaths could have been averted had access to doses not been hindered and had countries received them at scale earlier. Of the deaths averted in 2021 by COVAX vaccines, 153,000 were in never-Gavi countries, representing 18% of the total. By end of 2022, as COVAX supplies continued to ramp up significantly and it was able to reach more people in these countries, Imperial estimates that over 2.7 million deaths have been averted across AMC participants due to COVAX, with the total proportion of deaths averted attributable to COVAX rising to 34% across AMC countries (excluding India).
During a pandemic, the speed of the response is critical, especially given that research suggests that unvaccinated people are 11 times more likely to die from COVID-19 than vaccinated people. This implies that during the critical initial rollout, had vaccine hoarding and export bans not been such a hindrance to COVAX accessing supplies, more lives could have been saved in AMC-supported countries, particularly in the poorest countries.
Lives saved in LICs and Africa
When looking exclusively at low-income countries (LICs), the Imperial research suggests that COVAX averted a far higher proportion of deaths, 75%, over the period up to the end of 2022. In AMC countries in Africa, which historically have had very limited vaccine manufacturing capability and capacity across the region, where there have been 4 million confirmed cases and 63,000 deaths by the end of 2022, it was a similar story with COVAX helping to avert 73% of deaths during the same period. To date, COVAX has supplied nearly 550 million doses free of charge to African nations, making it by far the largest source of vaccines across the continent. It has also provided tailored support to increase uptake through technical assistance, cold chain equipment, training, and support for awareness campaigns.
What this suggests is that while all countries, irrespective of wealth, were able to benefit from equitable access to pandemic vaccines via COVAX, for the poorest nations, who had far fewer alternative routes to secure vaccines, COVAX served as a critical safety net. In addition to the poorest countries, the Gavi COVAX AMC has also been critical in providing a vital lifeline to never-Gavi countries that would have otherwise struggled to get access to vaccines.
The data also show how much more successful COVAX would have been had it not faced delays in accessing the large volumes of vaccines it had procured. Without vaccine hoarding by wealthier countries, export controls and manufacturing supply diversions and delays, more lives would undoubtedly have been saved, and more economic activity protected, across the AMC countries.
Key learnings
Despite the huge obstacles it faced and delays to global supplies of COVID-19 vaccines, COVAX was able to provide enough access to protect high-risk populations in many AMC countries. Given that there was no precedent for unified, multilateral responses to past pandemics – and no alternative global models in the current one – COVAX can be seen as a huge step forward in terms of harnessing global solidarity and towards vaccine equity.
COVAX’s unique experience offers key learnings in how equitable access can be achieved. Not only should it now be clear that anything that contributes to delay in providing access, particularly to low-income countries and African economies, will cost lives and cause severe economic damage, but also that a more equitable response is ultimately a better one for the world.
From COVAX’s experience, such delays could be avoided if there was:
- Increased regional supply resilience and manufacturing capacity of life-saving interventions, such as vaccines, particularly across Africa. This would go a long way to mitigate the vaccine hoarding and export restrictions that have so heavily hindered the free flow of vaccines during this pandemic.
- Transparency by manufacturers regarding their order books so that when delays occur or supplies are limited, it is possible to determine when countries that are unable to afford doses are in danger of disproportionally missing out.
- Contingency funding and surge capacity in place to enable global and regional health agencies to pivot during a global health crisis and mount a rapid global response. This is particularly important in countries that most need the support, to ensure they are not left at the back of the queue when it comes to procuring life-saving interventions, like vaccines.
- Mechanisms are in place that are designed to ensure that people in countries that are less able to afford life-saving interventions, like vaccines, therapeutics and diagnostics, get equitable access, particularly those people most at risk. Such mechanisms need to be in place before disaster strikes to ensure that valuable time is not lost creating them.
- A mapping out of existing global health solutions, mechanisms, networks, expertise, policies, frameworks and tools, including those created during COVID and retain, incorporate and evolve these as needed. This includes established innovations that have already proven to be critical in removing bottlenecks and speeding up the response time during COVID-19, such as Emergency Use Listing, indemnification and liability agreements and the No-Fault Compensation Scheme.
COVAX was not only a ship that was built as it set sail, but also one that has been adapted considerably since 2020 when it was first created. In 2022, as part of this ongoing adaptation to the challenges standing in the way of equitable access, COVAX has developed an innovative financing mechanism, the Pandemic Vaccine Pool, to ensure cash is on hand to make rapid procurement of this vaccines when necessary. Gavi, in partnership with the African Union, Africa Centres for Disease Control and Prevention (Africa CDC) and the G7 group of nations, is also developing a blueprint to foster and sustain an expanded vaccine manufacturing industry across Africa and other under-served regions of the world.
During a pandemic anything that contributes to delay in providing access to vaccines will leave people vulnerable, costing lives and economic damage. With COVID-19, the fact that a sizeable share of the vaccine doses received by both those countries that could not afford them and those that could came through COVAX, implies that this is true for all nations, irrespective of wealth. However, by far the greatest impact and benefit has been to LICs, particularly in Africa, because they are the ones that were more likely to have fewer alternatives. Therefore, given that the best possible global pandemic response is an equitable one, global future mechanisms should be designed particularly with these countries in mind.
References
© The Gavi Alliance. All rights reserved. This publication may be freely reviewed, quoted, reproduced or translated, in part or in full, provided the source is acknowledged.
The material in this publication does not express any opinion whatsoever on the part of Gavi, the Vaccine Alliance concerning the legal status of any country, territory, city or area or its authorities, or of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endor